Detect vision loss from ocular diseases
Simple, Reliable, Proven

ocular diseases without specialized training
Humphrey FDT is produced by the leader in diagnostic equipment for eye disease – Carl Zeiss Meditec
The Humphrey FDT® is from Carl Zeiss Meditec, the world leader in diagnostic test equipment for ophthalmology. Carl Zeiss Meditec is also the developer and distributor of the Humphrey® Field Analyzer, the recognized gold standard in visual field testing. Humphrey Field Analyzers are used by more eye care providers than any other automated diagnostic perimeter today.
Carl Zeiss Meditec, one of the world’s leading medical technology companies, offers integrated solutions for treating the four main eye diseases: vision defects (refraction), cataracts, glaucoma and retinal disorders. Diagnostic products range from slit lamps and fundus cameras to standard-setting diagnostic systems such as the Humphrey Field Analyzer, the Cirrus™ HD-OCT and the IOLMaster.® Carl Zeiss Meditec also produces surgical microscopes and innovative treatment systems for refractive laser surgery.
FDT can help your staff detect vision loss in
Clinically Validated
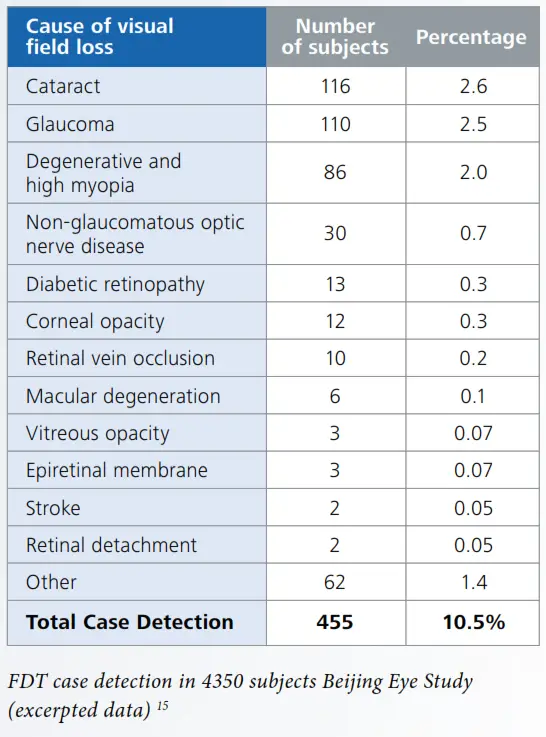
Multiple studies1-15 have shown that the Humphrey FDT detects visual field loss due to a variety of ocular diseases, including glaucoma. Thus FDT is ideal for clinics desiring to identify patients in need of ophthalmological referral.
• FDT is clinically validated in more than 170 peer-reviewed publications.
Proven Performance on Virtually all Patients
Studies have found that virtually all patients can perform this fast and simple test with reliable results:
• Beijing Eye Study: 98% patient success
• Tajimi Population Screening Study: 98.7% patient success.
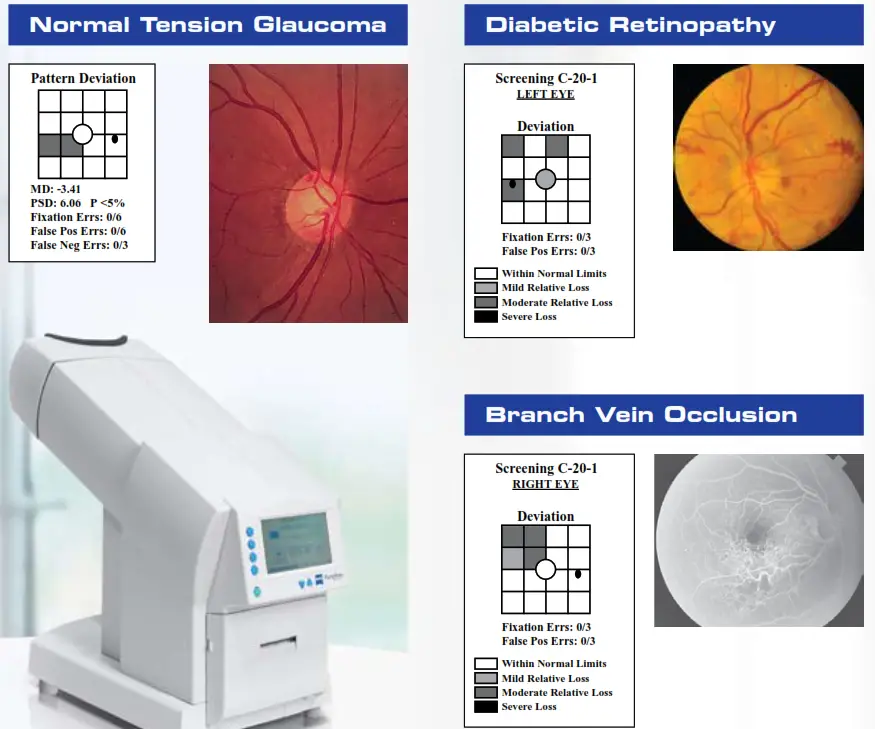
The Humphrey FDT can detect visual field loss
associated with a variety of ocular diseases

Ocular diseases without specialized training
Use the FDT Anywhere:
- General hospitals
- Polyclinics
- Community clinics
- Industrial health check clinics
- Optical shops
Patients with a positive FDT result can be referred for specialized ophthalmic examination. Interpretation criteria may be adjusted for local conditions.
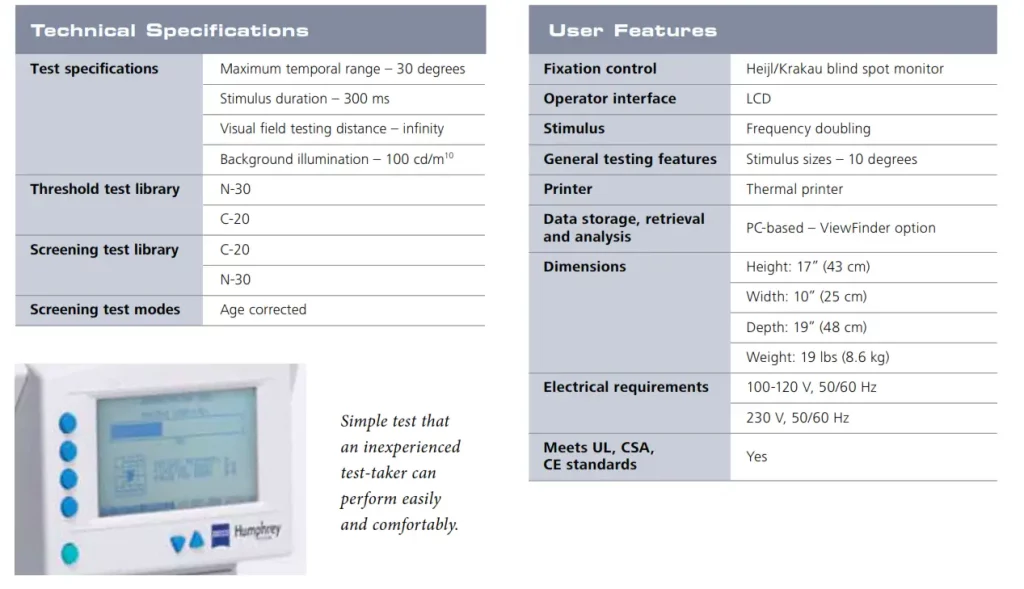
Easy to Operate and Interpret
The FDT is optimized for use in non-ophthalmological settings and may be operated by healthcare workers having little or no specialty training in ophthalmology.
- Simplified three touch operation
- Patients may be tested using their own glasses
- Short test: ~ 40 seconds per eye
- Small footprint
- Simplified interpretation of results

FDT is easy on patients
- Comfortable headrest
- Large, easily seen test stimuli
- Ergonomic response button
- Short testing time
The FDT is a small, automated peripheral vision testing device. The patient simply presses a response button whenever he/she sees a test stimulus. These simple perating requirements, coupled with the instrument’s well-documented clinical performance, make it a natural choice to detect the effects of eye diseases on visual function.
FDT is ideal for screening
-
-
-
-
-
-
- Highly sensitive in detecting visual field loss associated with a range of eye diseases
- Can be placed almost anywhere, including non-ophthalmic clinical settings
- Technician operated, with minimal training
- Fast and easy testing for patients in 40 seconds per eye
- Simple to understand test
-
-
-
-
-
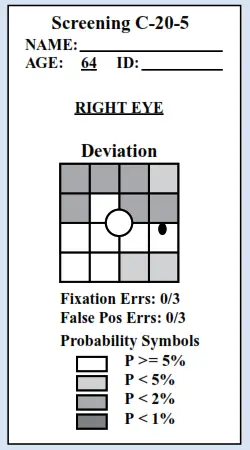
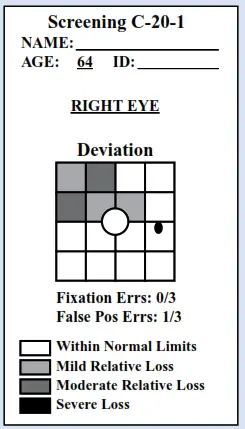 Shaded locations in the FDT printout indicate areas of visual field sensitivity that are outside normal limits.
Shaded locations in the FDT printout indicate areas of visual field sensitivity that are outside normal limits.
• The results illustrated above are consistent with a diagnosis of glaucoma. The darkest symbols indicate areas of the patient’s peripheral vision that were lower than that found in 99.5% of normal subjects.
The C-20-1 test emphasizes high specificity and is therefore best designed for general screening of large populations. The C-20-5 test emphasizes high sensitivity to optimize detection of early, subtle pathologic sensitivity loss, and is best designed for screening ophthalmic patients with risk factors or symptoms associated with eye diseases.
Humphrey FDT Perimeter
SAP# 000000-1781-970 FDT .2415 0909
The contents of the brochure may differ from the current status of approval of the product in your country. Please contact your regional representative for more
information. Subject to change in design and scope of delivery and as a result of ongoing technical development. © 2009 by Carl Zeiss Meditec, Inc. All copyrights reserved. Cirrus HD-OCT, Humphrey, Humphrey FDT and IOLMaster are either registered trademarks or trademarks of Carl Zeiss Meditec, Inc. in the United States and/or other countries. Printed in XXXX XM
Carl Zeiss Meditec, Inc.
5160 Hacienda Drive
Dublin, CA 94568
USA
Phone: +1 925 557 4100
Toll free: 1 800 342 9821
Fax:
+1 925 557 4101
[email protected]
www.meditec.zeiss.com/us
Carl Zeiss Meditec AG
Goeschwitzer Str. 51-52
07745 Jena
Germany
Phone: +49 36 41 22 03 33
Fax: +49 36 41 22 01 12
[email protected]
www.meditec.zeiss.com

Zeiss Opmi Lumera 700 With Integrated Intraoperative Oct
General Set up
Step 1: Perform Parfocality:
- Focus on cornea by looking at the CALLISTO eye screen on highest magnification
- Perform eye piece adjustment (Pupil distance, lens power compensation…)
- Lower magnification
Step 2

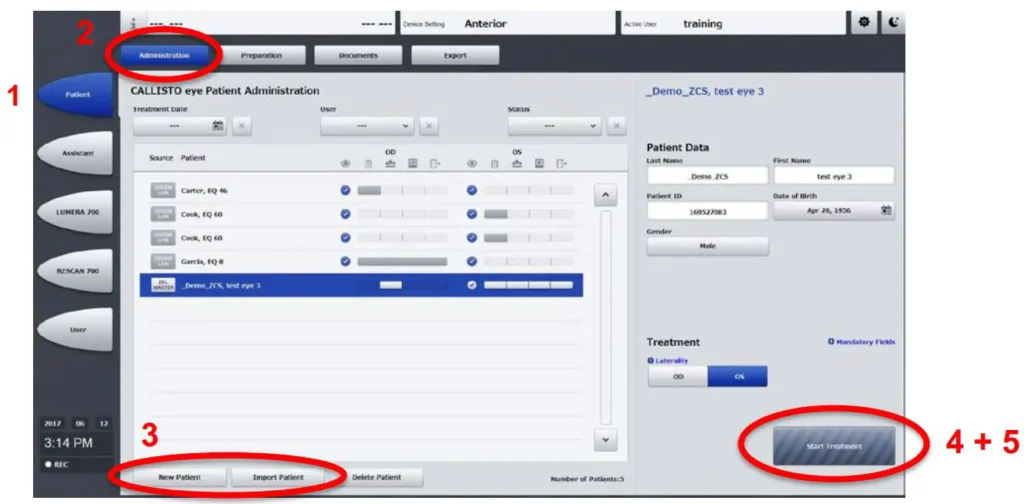
Anterior Set up
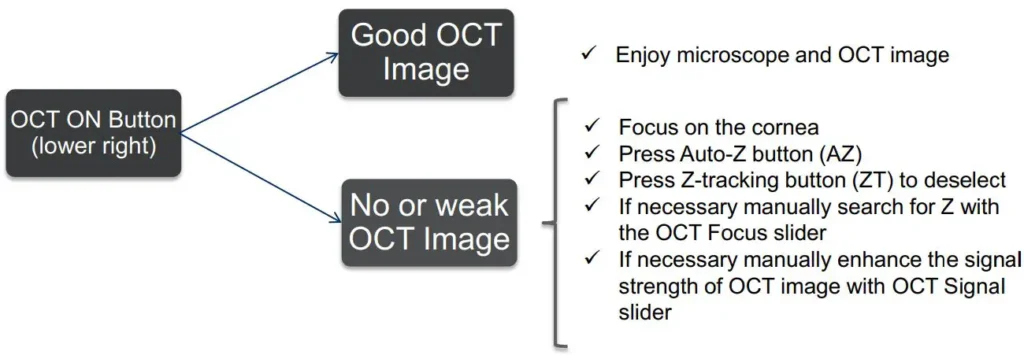
Step3
- Focus on the Cornea
- Activate OCT using the Foot Control Panel (FCP)
- Check if OPTIC icon anterior is activated(1)

- Use joystick on the FCP to set the scan location marker
Step 4
Posterior Set up
Step 5
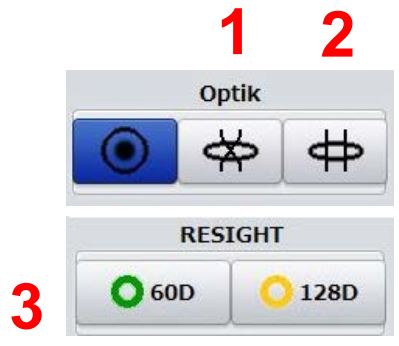
- Focus on the Cornea
- Choose optic icon: indirect lens(1) or direct(contact) lens(2) or if installed:
Slide in ZEISS RESIGHT 700 & chooserightlensicon128D (3)
Lower the ophthalmic lens of the ZEISS RESIGHT 700
- Focus on the retina
.When using the ZEISS RESIGHT 700 focus on the retina with the RESIGHT focus
Step 6
- Activate OCT with FCP
- Use joystick on FCP to set scan location marker
- Press Auto-Z button on the screen to find z plane and automatic tracking(ZT)
Step 7

Documentation
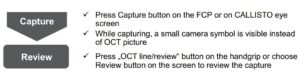

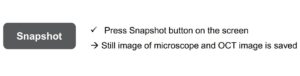



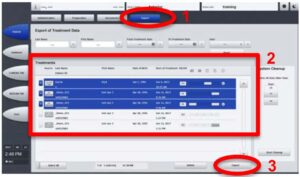
Export of Image / Video Data





Foot Control Panel –integrated intraoperative OCT active
FCP Standard
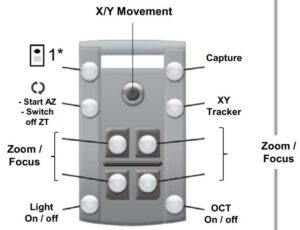
Standard FCP configuration. Use of joystick moves OPMI head in x/y direction–button left top does not need to be pressed.
FCP mode 2
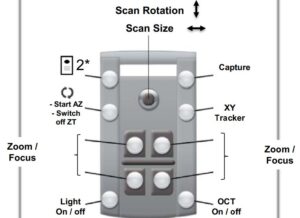
Second FCP configuration. Press button top left once, then use of joystick changes scan rotation & size.
FCP mode 3
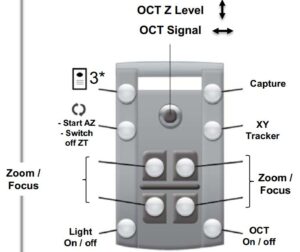
Third FCP configuration. Press button top left twice, then use of joystick changes OCT Z level & OCT signal.
Read More About This Manual & Download PDF:
Zeiss Opmi Lumera 700 With Integrated Intraoperative Oct User Manual – Optimized PDF
Zeiss Opmi Lumera 700 With Integrated Intraoperative Oct User Manual – Original PDF
Questions about your Manual? Post in the comments!
References
]]>
Recommended Protective Coverings
With the health and safety of you, your patients and your staff in mind during the COVID-19 pandemic, ophthalmic practices are advised to take extra precautions to prevent the spread of germs by using protective coverings on equipment when at all possible.
Forehead Rest
Start with the forehead rest cover.
Chinrest
Next, cover the chinrest.
Handle Grips, Mouse and Keyboard
Lastly, cover handle grips, keyboard and mouse.
Using a single-use protective covering may help put your patient at ease and demonstrate your commitment to their health and well-being. Below, you’ll find a list of suggested protective products to help facilitate a hygienic environment.
These products are recommended to be used as single-use disposables and should be changed after each patient visit. Simply slip the sleeves on before the patient arrives, and remove and replace them before your next patient exam.
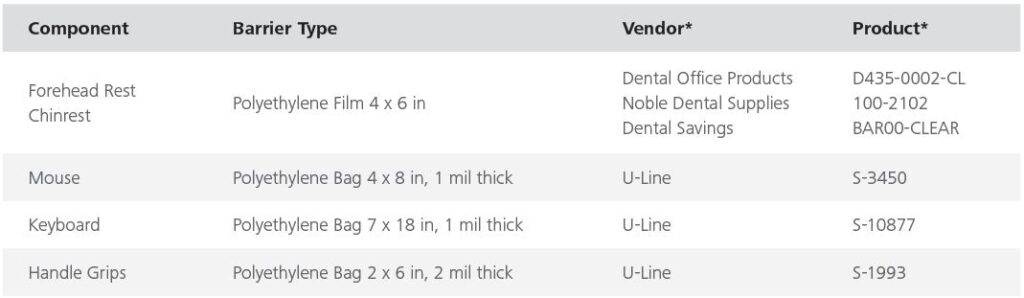
*Suggested protective coverings are not sold with ZEISS products. Examples shown are select U.S. vendors, which may not be available in your market.
You may find comparable vendors in your own market.
Please always refer to User Manual for any further instruction on operation of device.
EN_31_025_0397II; CIR.12329 Rev B ©Carl Zeiss Meditec, Inc. 2020. All rights reserved.
Zeiss Cirrus Oct Family Recommended Protective Coverings Instruction Manual – Optimized PDF
Zeiss Cirrus Oct Family Recommended Protective Coverings Instruction Manual – Original PDF
References
]]>SPIEDigitalLibrary.org/conference-proceedings-of-spie
SEM AutoAnalysis for reduced
Kokila Egodage, Fan Tu, Horst Schneider, Christian F.
Hermanns, Grizelda Kersteen, et al.
Kokila Egodage, Fan Tu, Horst Schneider, Christian F. Hermanns, Grizelda Kersteen, Bartholomaeus Szafranek, Kristian Schulz, “SEM AutoAnalysis for reduced turnaround time and to ensure repair quality of EUV photomasks,”
Proc. SPIE 11147, International Conference on Extreme Ultraviolet Lithography 2019, 111471G (26 September 2019); doi: 10.1117/12.2538474
 Event: SPIE Photomask Technology + EUV Lithography, 2019, Monterey, California, United States
Event: SPIE Photomask Technology + EUV Lithography, 2019, Monterey, California, United States
SEM AutoAnalysis for reduced turnaround time and to ensure repair quality of EUV photomasks
Kokila Egodage*a, Fan Tub, Horst Schneiderb, Christian F. Hermannsb, Grizelda Kersteenc, Bartholomaeus Szafranekb, Kristian Schulz a
aCarl Zeiss SMT GmbH, Carl-Zeiss-Promenade 10, 07745 Jena, Germany; bCarl Zeiss SMT GmbH, Industriestrasse 1, 64380, Rossdorf, Germany; cCarl Zeiss SMT GmbH, Rudolf-Eber-Strasse 2, 73447, Oberkochen, Germany.
ABSTRACT
With the semiconductor industry tending towards adding multiple layers consisting of EUV technology in high-end manufacturing and the production of many EUV scanners to meet customer demands, novel approaches for EUV defect review are being readily investigated. The successor of the quasi industry standard AIMS™ and sole actinic defect
review tool available currently is AIMS™ EUV. As the industry already introduced this newcomer in the manufacturing environment, other steps in the workflow were forced to adapt to the new technology. One example is the automated aerial image analysis process where the DUV aerial image analysis software, AIMS™ AutoAnalysis (AAA), was enhanced for the EUV solution in order to handle high resolution EUV images. This was a necessary step for full automation similar to the process achieved with AIMS™ and AAA.
Another important domain in the back end of line is defect repair where the e-beam based repair tool MeRiT® is also the quasi standard in the mask manufacturing industry especially for high-end photomasks. After undergoing changes to keep up with shrinking feature sizes and complex repairs MeRiT® tools were able to overcome these challenges and fulfill the current industry demands and expectations. For mask makers timely supply of error free high-quality masks is of the essence which can be further ensured by introducing a higher level of automation to the repair workflow.
Following a similar approach to the optical counterpart, a digital solution known as SEM AutoAnalysis (SAA) has been developed. With SAA, a quick and fully automated SEM image-based quality assessment after a repair of a photomask is readily achievable. Moreover, the repair technicians benefit vastly by having the complete repair history of a defect for their decision-making process which would lead to a reduction of the turnaround time. As a consequence, unnecessary time wastes during mask un/loading cycles can be avoided.
The myriad data produced in the BEOL, originating from different modalities, can be converted to meaningful information with the help of automation enabling technicians to make better decisions, reducing the risk of mishaps, improve repair quality and reliability of processes in general. Since mask defects that go through each tool are the same, data produced by different tools should retain that common denominator for an efficient assessment. This assessment needs to be applied to the areas of different modalities where a comparison is possible that led to the investigations to test the feasibility of combining SEM and EUV data. A comparison of SAA results with AIMS™ EUV measurements analyzed with AAA on the same photomask and defects are presented along with this proceeding. The results show that SAA can provide a valuable preliminary assessment of photomask repairs. Nevertheless, due to the nature of SEM based analysis, AIMS™ EUV technology remains mandatory for a final mask repair qualification and a complete specification check, i.e. mask repair verification. The outcome of this investigation paves the way towards a fully automated BEOL where different workflows and data originating from several tools in the mask shop can be interconnected and controlled.
Keywords: SEM AutoAnalysis, AIMS™ AutoAnalysis, EUV, SEM, aerial image, MeRiT®, AIMS™
INTRODUCTION
Since the introduction of EUV in the semiconductor industry most of the major players have been gradually incorporating changes to their already well-established processes in mask shops to accommodate the newcomer. Within the past few years major investigations were carried out to find the most appropriate EUV blanks as well as pellicle material. Currently these investigations are being continued to achieve better line edge/width roughness, reduced number
of defects and durable/sustainable photomasks [1, 2]. Furthermore, multi-patterning appears promising as it brings sub- 50nm features onto masks [3]. As a result, tighter specifications are applied that essentially increases the number of defects on reticles. Keeping the latter at bay is vital because a single particle can have negative repercussions in terms of the wafer yield [4]. Therefore, the defect review sector in the BEOL welcomed the AIMS™ EUV tool that successfully captures high resolution images compensating for the decreasing feature sizes. This forced mask makers to make necessary adjustments in the mask shops emphasizing its importance for production.
Reflecting upon this experience, mask shops would have to optimize processes in the BEOL to quickly adapt to changes and customer demands. Using smart automation especially when faced with smaller specifications and increasing number of defects, would be one way to adapt to changing conditions. The need for such a solution is seen by the
persistently high turnaround time (TAT) at smaller nodes in the past couple of years [5]. The complexity of masks also worsens the situation as the sub-resolution assist features (SRAFs) would reduce to 32-40 nm [6]. Considering the current working scenario in the BEOL even having a handful of defects on the mask can mean many un/loading cycles
before the mask is defect free. To combat this trend, an industry proven solution offers the use of data-connectivity and automation in a well-designed architecture that is both flexible and stable. It utilizes a software known as AIMS™ AutoAnalysis (AAA) that carries out automated defect analysis and produces a comprehensive report with desired level of detail [7]. Direct connection with the AIMS™ tool via the FAVOR® system enables parallel defect analysis once both aerial reference and defect images are available. This not only minimizes operator involvement avoiding any mishaps but also allows the flexibility to view analyzed data directly after measurements. The application works in a modular fashion that enables changes quicker than in any other arrangement. For example, the internal working segments of the software such as analysis recipes and report templates can be easily modified and attached to specific analysis jobs that would function untouched until needed. As expected the inclusion of AAA in the BEOL has reduced the time taken during the repair-review cycles, reduced misclassifications and enabled a comprehensive analysis of defects and repairs [7]. Similarly, EUV defect review benefits from this software solution that would keep the TAT from exploding. AAA has
undergone changes to adapt to specific EUV applications i.e. the ability to cope with large data traffic produced by the high-resolution aerial images captured by the AIMS™ EUV tool. Such capability promotes smaller yet different defect types to be spotted at a quicker pace without wasting operator time.
The defects that occur on EUV masks are clearly different to that encountered with that of DUV due to the multilayer structure of the former. The defect types range from phase defects, translated from the substrate through the multilayer, to regular hard defects which occur during fabrication [1, 2]. Contamination can always occur during any application step and these repairs strongly impose on-time tool adaptability. The MeRiT® tool has overcome this challenge and successfully displays the capability to repair EUV defects taking the lead in this domain. To extend the level of automation from defect review to repair, single MeRiT® tool preparation steps have been automated that essentially frees the operator to carry out other tasks while the processes run. Following the footsteps of the aerial domain implementation, the software SEM AutoAnalysis (SAA) enables the automatic analysis of defects and post-repairs after each image acquisition. Initially, steps to customize analysis recipes and report templates must be carried out for each feature type but after the initial time investment the prepared modular components can be readily used for later jobs. This would save a lot of time in the long run. SAA gives the operator a detailed overview of the defects that can be compared against the specifications and assists in arriving to a decision regarding the type of defect and the subsequent effects on the mask. The operator is provided with tangible results to assist in realizing the kind of repair and defect severity. Compared to the aerial version, completely different algorithms are used for SEM image processing given the native differences between the two image types. Furthermore, analysis strategies have been specially modified and designed to fit the use cases which will be mentioned in the methodology.
SAA in combination with the repair tool MeRiT® brings many advantages to mask shops. The feature in MeRiT®, known as SEM Review, together with SAA can in fact replace long term costs of maintaining a separate tool for bulk defect capture as it enables automated imaging of defects including navigation and autofocus. Intermediate steps until the repair can also be implemented elsewhere freeing the tool for more measurements. Uncomplicated repairs can be carried out automatically with the option for manual intervention whenever needed via the MeRiT® feature Advanced AutoRepair.
This leads to improved repair quality and process reliability in the repair regime. The fact that SAA is able to use images that are automatically grabbed by the tool during repair makes it easy for the user rather than capturing extra images for a third-party software.
For a complete assessment of repairs, data from more than one modality is always useful since they assist in making better decisions. Taking mask defects into account, the repair and review processes contain the common aspect that their local coordinates are identical even though imaged through two different modalities. Currently data from these two modalities are handled separately that would lead to ~35% of time being wasted compared to that with repair optimization and disposition automation [8]. There are measures taken via machine learning to close this gap, for example, by using one image type as input and predicting the other but these studies are still in the research phase and not ready for high-volume manufacture [9, 10].
Focusing on the repair verification loop, the data commonly used are SEM and aerial images. As a first step towards the accurate alignment of both EUV and SEM images systematic investigations were conducted where both AAA EUV and SAA were used for image analysis, respectively. This led to a comparison between the two types of data. Both lines and spaces and contact hole images were captured using a ZEIS internal mask. Given the nature of both modalities the conditions for assessment were varied as thought fit. These are the preliminary steps in the BEOL towards a fully connected mask shop that leverages the vast amount of data produced automatically on a daily basis.
1.1 Comparing Aerial and SEM imaging
Similar to all imaging methods aerial and SEM imaging both have dedicated tools with preparation/calibration steps that are very different to one another. If these tool preparation steps are not followed accurately the images can have undesirable side effects. The AIMS™ tool was mainly developed to detect defects and all related processes are optimized to reflect the final wafer printability. The four times magnification from wafer to mask causes errors, present on masks, to be transferred to wafer and this ratio, known as mask error enhancement factor (MEEF), leads to defects that are larger on wafers than on masks. This ratio is small for EUVL compared to that of 193i [11]. This behavior however does not persist in SEM images since imaging is carried out one-to-one at the mask as the MeRiT® tool was initially developed for repair or defect review purposes. Therefore, estimating printability is difficult only using SEM images, other than developing other methods include simulations.
In terms of detecting phase defects aerial imaging is at the forefront. With the help of Bossung plots through-focus variations can be readily identified [12]. On the contrary, phase defects are not visible on SEM images as the secondary electrons, generated during the interaction of the primary beam and the substrate, can produce the same intensity in the defect and the unaffected areas. This difference between the two modalities is simply due to the principles of the imaging tools. Another aspect, as a result, is that the SEM images magnify roughness information compared to that with aerial. Due to the high resolution of SEM images, more information of the line width roughness is captured which can be used for further detailed analysis of the mask. The resolution of AIMS™ EUV is at its best for an optical system. As published by Chen et al. the line width roughness between AIMS™ EUV and SEM resists behave as similarly [13]. This leads to the conclusion that SEM defect detection can be considered as an inspection tool that detects very many variations that can be later be filtered. Especially with the lack of inspection tools for EUVL, defect detecting methods using SEM images is an asset to the BEOL.
METHODOLOGY
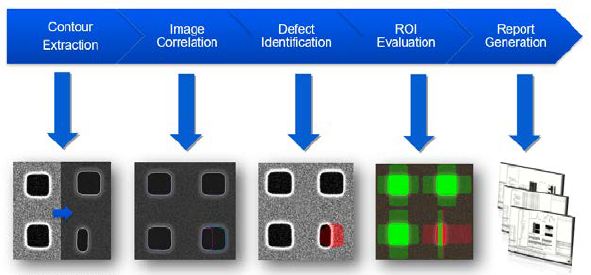
Since two completely different modalities are being compared, i.e. SEM and aerial, the test implementations were aligned and adjusted with one another. As for our image data set two feature types were investigated i.e. periodic lines and spaces patterns and periodic contact hole patterns. For defect identification a reference image with no defects is required to compare with the defect image. The only restriction on the software is that the image sizes should be the same. There are various contour extraction algorithms available that fit to different mask/feature types and the contour extraction parameters can be manually edited to obtain perfect contours. This is the heart of the software as all the following steps depend on the contour extraction. Another feature that is applicable for post repair images is the cropping function enabling the software to only focus on a specific region. As post repair SEM images contain DC dots that can be falsely detected as a defect the above function is very useful. Then both reference and defect images are correlated followed by the defect identification step. Furthermore, a more detailed analysis is conducted depending on the criteria given on the analysis recipe. Finally, a comprehensive report can be produced with user defined filters to emphasize desirable data. All the above steps of the SAA software workflow are depicted in Figure 1.
Images captured must also be suitable in terms of quality. The MeRiT® captures images with sufficient resolution and good quality with respect to noise levels, contrast and roughness. This is the same for AIMS™ EUV tool and the image analysis workflow in AAA which is the same as described for SAA.
Lines and Spaces patterns
In total 12 image pairs were analyzed of which 10 are 68nm half pitch lines and spaces and contained 7 nm extrusion defects (please note, that all dimensions are on mask level). Moreover, post repair images of a 68 nm single and a triple bridge with a length of 1000 nm along with relevant reference images for both SAA and AAA were considered. The
images were 4500 × 4500 nm2 with a resolution of 3000 × 3000 pixels and the post repair SEM images contain DC dots.
First, the behavior of CDs between the two modalities were investigated. A larger area on SEM images, 1898 × 1489 nm2, was chosen due to the larger line edge/width roughness compared to aerial images, 1194 × 411 nm2. These results were used for an initial analysis of the approximate range of the CD values in the SEM and aerial images.
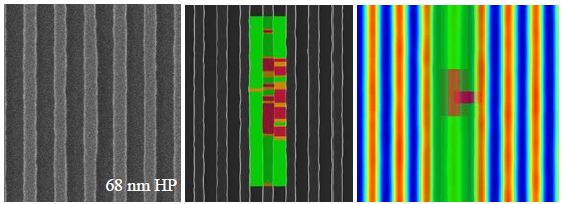
Then, the line-line comparison produced a more detailed investigation. Figure 2 shows an image set showing the raw SEM image with a 7 nm programed extrusion defect (left). Note: the center line is slightly wider than the neighbor lines.
After processing with SAA, a contour extracted image overlaid with CD variations can be obtained (middle). The color coding represents failing (red) and critical (orange) regions. This categorization can be customized in the analysis recipe and for this case the failing regions represent > ±10 % and critical regions > ±8 % CD deviations. The aerial image on the right is the variant of SEM but only shows pass and fail regions for simplicity.
Contact Hole patterns
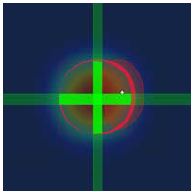
For the contact hole data set 6 image pairs were considered. The contact holes were 140 nm in edge length and each image was 3000 × 3000 pixels. The distance between each contact hole in X and Y is 200 nm (outer edge- outer edge). The defect types were varying: 1 missing and 5 half missing contact holes. Figure 3 displays a sequence of images that represent the analysis criteria possible with contact holes. Besides the CD widths, the area of the reference and defect contact holes can be compared. In addition, the placement of the contact holes at specified angles can be evaluated with respect to the reference image. Figure 3 D shows this clearly as the placement is calculated at 0, 45 and 90 degrees.
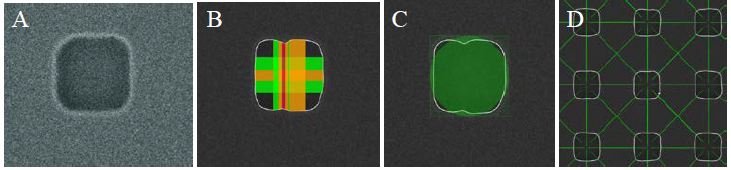
Due to the difference in optical resolution of the AIMS™ EUV the contact holes seem rounder than that on SEM images. With the help of the analysis recipe only a narrow region was used for analysis (Fig 3. B and Fig 4.), both vertically and horizontally (Fig 4.). Of course, more directions are possible, but we took only two directions for simplicity. AAA/ SAA automatically detects any area deviation when analyzing contact holes and this is depicted with the red blob in Figure 4. The slices do not show any defect since the horizontal CD width comparison results in a pass with respect to the applied tolerance criteria.
RESULTS AND DISCUSSION
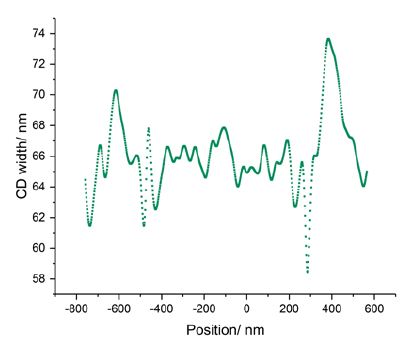
During the investigations the measurement metric was varied between SEM and aerial images mainly to compensate for the natural difference in the two image types. Especially with SEM images that captured more rugged topological information, post processing steps such as smoothing and alignment of plots in x- and y-axis were applied when necessary. Figure 5 shows the raw SEM CD values across a 68 nm single bridge post repair which is far more volatile compared to AIMS™ EUV data shown in Figure 8 (red).
Lines and Spaces patterns
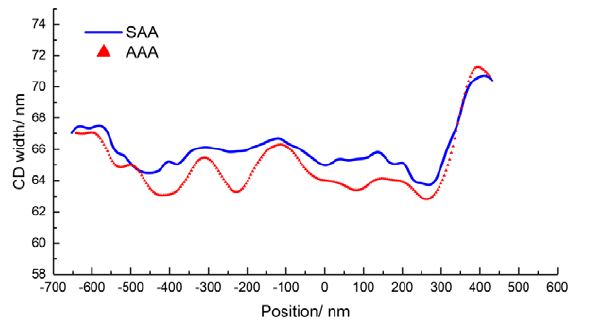
Given the large line width roughness in SEM images, a larger area on the SEM image was considered for an initial comparison. This resulted in an interesting trend where the CDs from the aerial image was well nested within the values extracted from the SEM image. Figure 6 displays the CD widths of three neighboring lines on AIMS™ EUV and SEM
images. The CD widths were extracted using both AAA and SAA, respectively. The SEM CD widths are within the standard deviation of AIMS™ EUV values.
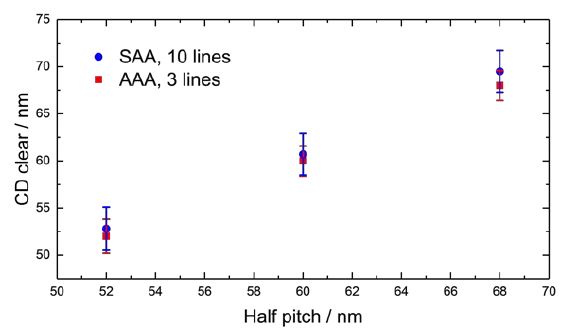
The discrepancy between the two values relates to the differences mentioned in section 1.1. which leads to the conclusion that SAA can detect more variations.
When comparing CD deviations observed in SEM and AIMS™ EUV images a similar trend surfaced. Average CDs of the repaired area in the post-repair image were compared with the average reference CDs. Taking the average specially for SEM images enabled to have a more comparable statistics and minimized the effects of the high line edge/width roughness (Figure 7).
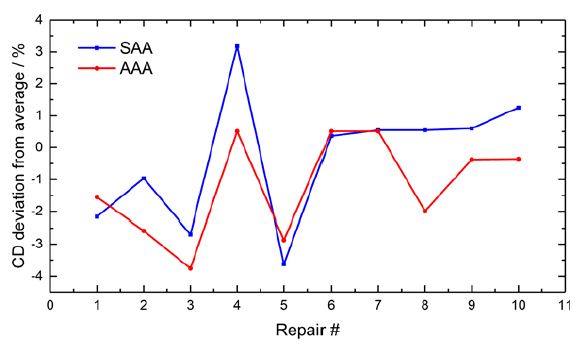
CD widths extracted from SEM and aerial images proved the above observation further. The results from SAA (blue) shown in Figure 8 and 9 are processed using a smoothing filter to be able to compare with the aerial images. This compensates for the native roughness levels of SEM images. Vertical and lateral adjustments to the plots were necessary for clarity and adjust for the differnce stage alignment between two tools. Figure 8 shows the comparison of a 68 nm single bridge defect after repair whereas Figure 9 is that of a 68 nm triple birdge defect.
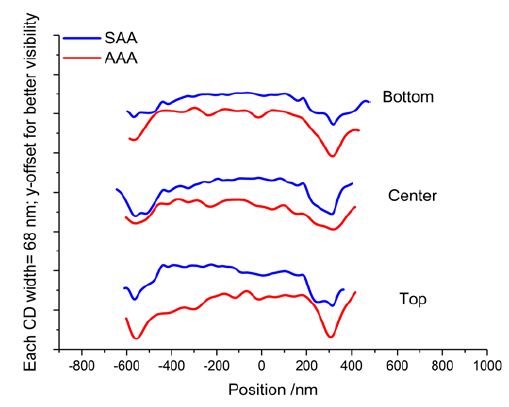
are shown separately for clarity.
Smaller scale analysis, i.e. only considering single lines and CD widths, shows similar variations between both modalities even though expectedly raw SEM plots show more peaks compared to that in aerial images (Fig 5.). The peaks align considerably well between SAA and AAA results. However, the variability between the two is quite large and this matching depends on the quality of the repair. With the triple bridge example, it can be seen that a repair taking place in close vicinity could affect the variability of SEM data. However, SAA and AAA data show similarities between -600 – 400 nm and 200 – 400 nm.
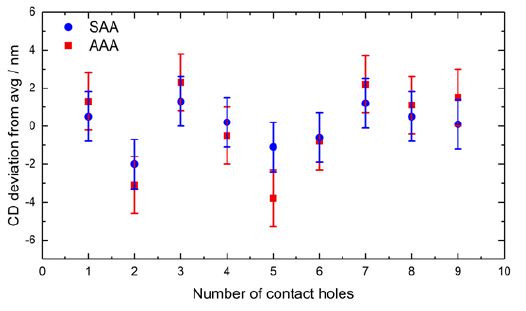
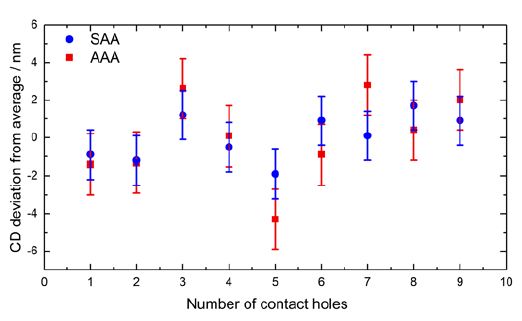
Contact hole patterns
Both vertical and horizontal CDs were measured with the focus on one simple post-repair defect where the middle contact hole was missing. The contact holes surrounding this etch were also analyzed and all data are plotted in Figures 10 and 11. The CD deviation from average was compared between both SAA and AAA results. For better comparison between the two images the threshold of AIMS™ EUV results was increased by 16.7%. This allowed to take the average CD deviation in both cases and the tolerance criteria were kept the same for both modalities i.e. at >±8% fail and >±5% critical. AAA had identified a defect at the right edge of the repaired contact hole (Fig. 4) due to the differences in area between reference and post-repair images even though the result status was labelled pass, whereas critical for SAA.
SUMMARY AND OUTLOOK
For the efficient reduction of TAT in the back-end of mask manufacturing many time-consuming intermediate steps, such as queueing, loading and unloading masks and shuttle time, between MeRiT® and AIMS™ EUV systems were addressed by comparing their SEM and aerial images, respectively. The results show that the CD widths as well as CD deviation measurements follow a similar trend with SEM and AIMS™ EUV images. The entire analysis was carried out via the software SAA and AAA, respectively. Despite using different analysis algorithms, the trends were visible. This leads to the conclusion that SAA data is not an exact match to that of AAA but comparable and demonstrates a similar trend. Industry in fact needs AIMS™ EUV for flawless defect disposition and verification.
If such an implementation were to enter mask shops, an all-inclusive data connectivity is achievable. Having access to complete data sets that the MeRiT® and AIMS™ EUV tools produce, these preliminary efforts can be further improved to a product that shows a relative verification after a defect repair. This enables technicians to make quicker and reliable decisions when estimating the quality of a repaired defect. Moreover, with the lack of an actinic pattern mask inspection tool for EUVL, SEM images are a great resource. AIMS™ EUV being bulky and expensive, though the gold standard of defect verification, this implementation is seen as a bridging technology until the EUV verification tool reaches the mask shops.
Besides the comparable analysis results of SAA and AAA, both applications provide an automated way of evaluating SEM and aerial images within a short time and an improved reliability in comparison to even experienced operators [7]. To further extend the degree of automation with all its benefits as well as the correlation to other tools and data types, a similar investigation as presented here is necessary. All captured data can then be collected and viewed on the overarching solution, Advanced Repair Center (ARC), which further enhances the efficiency and reliability of mask shops.
ACKNOWLEDGEMENTS
We would like to thank Dr. Dmitry Simakov, Dr. Renzo Capelli, Dr. Michael Waldow and Matthias Stecher for fruitful discussions.
REFERENCES
- Rastegar, A., Jindal, V., “EUV mask defects and their removal”, Proc. SPIE 8352, 83520W (2012).
- Huh, S., Ren, L., Chan, D., Wurm, S., Goldberg, K., Mochi, I., Nakajima, T., Kishimoto, M., Ahn, B., Kang, I., Park, J., Cho, K., Han, S., Laursen, T., “A study of defects on EUV masks using blank inspection, patterned mask inspection, and wafer inspection”, Proc. SPIE 7636, 76360K (2010).
- Simone, D. D., Singh, A., Vandenberghe, G., “Printability study of EUV double patterning for CMOS metal layers”, Proc. SPIE 10957, 109570Q (2019).
- LePedus, “EUV mask gaps and issues”, Semiconductor Engineering, 8 May 2019,
https://semiengineering.com/euv-mask-gaps-and-issues/ (4 July 2019) - eBeam Initiative, “Mask Maker Survey”, 18 September 2018, https://www.ebeam.org/docs/eBe.am-Mask-Maker-Survey-2018.pdf (24 July 2019).
- LaPedus M., “More EUV mask gaps”, Semiconductor Engineering, 17 November 2016, https://semiengineering.com/more-euv-mask-gaps/ (25 July 2019).
- Russell, G., Jenkins, D., Goonesekera, A., Dornbusch, K., Sargsyan, V., Zachmann, H., Buttgereit, U., “Automated defect disposition with AIMS AutoAnalysis”, Proc. SPIE 10451, Photomask Technology, 1045113 (2017).
- Schulz, K., Egodage, K., Tabbone, G., Garetto, A., “How smart is your BEOL? productivity improvement through intelligent automation,” Proc. SPIE 10454, 104540X, (2017).
- Bürgel, C., Sczyra, M., Utzny, C., “Necessity is the mother of invention: support vector machines for CD control”, EMLC Dresden, VDE, (2019).
- Evanschitzky, P., “Mask defect assessment from SEM images aided by deep learning methods”, EMLC Dresden,VDE, (2019).
- Walia S., [Low Power Semiconductor Devices and Processes for Emerging Applications in Communications, Computing and Sensing] CRC Press, Boca Raton, 5-6, (2019)
- Garetto, A., Uzzel, D., Magnusson, K., Morgan, J., Tabbone, G., “Utilization of AIMS Bossung plots to predict Qz height deviations from nominal,” Proc. SPIE 8886, 88860K (2013).
- Chen, X., Verduijn, V., Wood, O., Brunner, T., Capelli, R., Hellweg, D., Dietzel, M., Kersteen, G., “Evaluation of EUV mask impacts on wafer line-edge roughness using aerial and SEM image analyses,” Proc. SPIE 10583, 105830J (2018)
Spie SEM Auto Analysis for reduced turnaround time and to ensure repair quality of EUV Photomasks Instruction Manual – Optimized PDF
Spie SEM Auto Analysis for reduced turnaround time and to ensure repair quality of EUV Photomasks Instruction Manual – Original PDF
References
]]>Social distancing with your ZEISS HFA3: Extended cable connection

What you’ll need for extended connection
- Additional video display – Standard Monitor, TV, or Projector capable of handling 1024×768 video resolution, 60Hz refresh rate, with one of the video display interfaces described below.
- Monitor cable: recommend limit length to 5 meters, or less
– HFA3 side: Passive DisplayPort or VGA.
– Monitor side: appropriate connection for additional monitor. - USB keyboard and mouse – choice of: wireless or wired.
- Extender to achieve social distance length if using wired option.
Disclaimers
- The following suggestions are not intended as a comprehensive solution for managing the clinical workflow in ophthalmic offices as related to COVID-19 virus (or similar) management.
- Any cables used for connecting additional video displays and extended peripherals should be routed and safely secured to avoid any potential tripping hazards.
- With the exception of peripherals available from ZEISS with the HFA, specific video display devices and peripherals are not guaranteed to have been tested or verified by ZEISS. Some video displays may require adjustment of the native display graphics configuration.
- It is recommended that the lengths of any extension cables used are limited to a maximum of six meters (19.7 ft) to ensure reliability.
- All periphery devices are not sold by ZEISS and is customer responsiblity.
Steps to connect display and peripherals to ZEISS HFA3
Connecting an additional monitor and peripherals to HFA3
- Remove the back panel of the HFA3 and locate an available video port.
Note: Two different computer models have been used with HFA3 that have different port configurations (CPC and Mini ITX). - Connect a second monitor to the HFA3 using the available video port(s).
- Position the second monitor an extended distance away from the HFA3.
HFA3 (CPC model) – serial numbers below 8×0-15000
Video Signal: 1024 x 768, 60 Hz, (4:3 Aspect Ratio) Dual Monitor Mode: Mirror
External displays can be added to the following port(s): 1 DisplayPort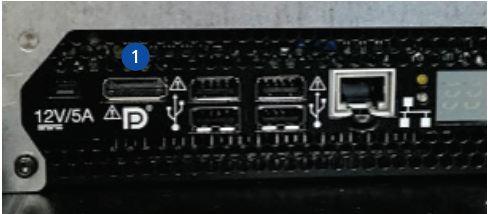
HFA3 (Mini-ITX model) – serial numbers higher than 8×0-15000
Video Signal: 1024 x 768, 60 Hz, (4:3 Aspect Ratio)
Dual Monitor Mode: Mirror External displays can be added to the following port(s):
1 DisplayPort (Use this one)
2 DisplayPort (Do Not use this one)
3 VGA (OK to use but not preferred)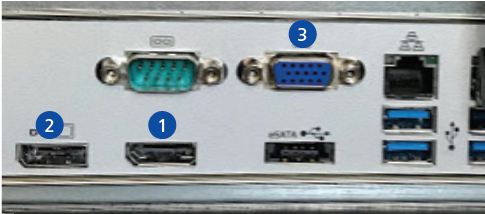
Video Extension Cable Options for HFA3
- DisplayPort cables – (preferred type) recommend 5 meters, or less, due to monitor specification limit.

- VGA cables – recommend 5 meters, or less. Signal quality could be affected.

Note: Do not use HDMI type connector. Not compatible with HFA3.
Connecting (or Extending) keyboard and mouse to HFA3
- Wireless keyboard or mouse within acceptable range as described by manufacturer (typically ~ 10meters).
– Logitech K830 wireless Keyboard + Touchpad device was used in testing at Zeiss. Also sold as an option with HFA3.
– Connect wireless USB key into any available USB port on HFA3 (Operator interface panel has 2 USB ports). - Wired USB keyboard and USB mouse with extended cable
– Connect to any available USB port on HFA3 (Operator interface panel has 2 USB ports).
– Most off-the-shelf keyboard and mouse products are compatible with HFA3.
Notes:
- Wireless Keyboards: Logitech K830 keyboard (2.4GHz) = wireless range: 10m
- Wireless Mice: Logitech M525 mouse (2.4GHz) = wireless range: 10m
- Wired Keyboard / Mouse Extension Options: Passive USB extension cables recommend limit length to 6 meters, or less
For additional guides on social distance cable set-up with your HFAII-i or other ZEISS diagnostic devices, please visit our MED Support Now page, www.zeiss.com/med-support-now.
Zeiss Humphrey Field Analyzer 3 [HFA3] User Manual – Optimized PDF
Zeiss Humphrey Field Analyzer 3 [HFA3] User Manual – Original PDF
References
]]>
ZEISS DeepRecon
Faster 3D X-ray imaging throughput and superior imaging quality
for advanced package analysis
ZEISS DeepRecon is the first commercially available deep learning reconstruction technology in the 3D X-ray imaging market.
Intended for applications that repeatedly analyze the same or similar sample types, DeepRecon enables faster 3D X-ray scans while preserving ZEISS’s revolutionary Resolution at a Distance (RaaD) and image quality advantages.
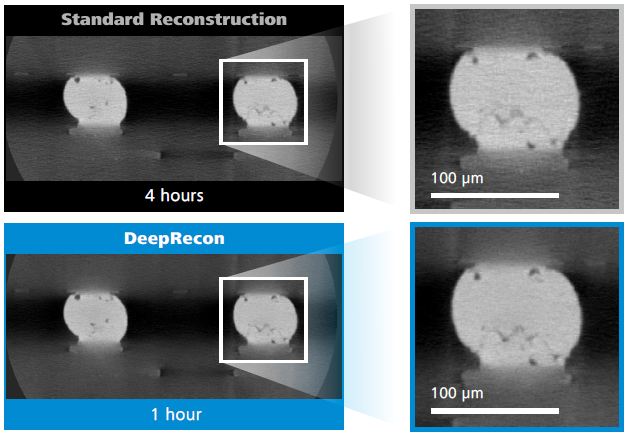
Faster Throughput by up to 4X
Rapid structural and failure analysis (FA) aids fast product introductions and high customer satisfaction levels. Shrinking package interconnects, higher packing densities, and increasing package sizes result in smaller, more difficult-to-find defects and longer analysis times. DeepRecon enables faster high-resolution, high-quality 3D X-ray image acquisition for repetitive workflows used in process development and quality control. Up to 4X faster throughput is possible by leveraging deep learning networks customized per package type. The result is faster time to results and ability to increase sampling rates – all
achieved without increasing the radiation dose to the sample.
Better Image Quality
High image contrast, high resolution, and high signal-to-noise ratios (SNR) are needed to produce the highest quality images for improved visualization of defects and small or low-contrast features. To achieve a high SNR using standard reconstruction techniques, higher exposure times and/or projections are generally required, which can significantly impact throughput. DeepRecon offers a statistically improved SNR, providing superior image quality. DeepRecon also reduces image artifacts that are typically inherent in faster imaging processes.
Customized, Optimal Performance
DeepRecon is a workstation-based option offered as a special customer solution for
ZEISS Xradia Versa X-ray microscopes (XRM) and Context microCT instruments. Network models are created per sample “class” and can be tailored to precisely fit targeted repetitive applications, enabling an ideal balance of image quality and throughput. Available for new or existing systems, the DeepRecon option uniquely opens opportunities in big data generated by 3D X-ray and provides significant AI-driven speed or image quality improvement.
DeepRecon is offered via the unique Advanced Reconstruction Toolbox for ZEISS Xradia 3D X-ray systems.
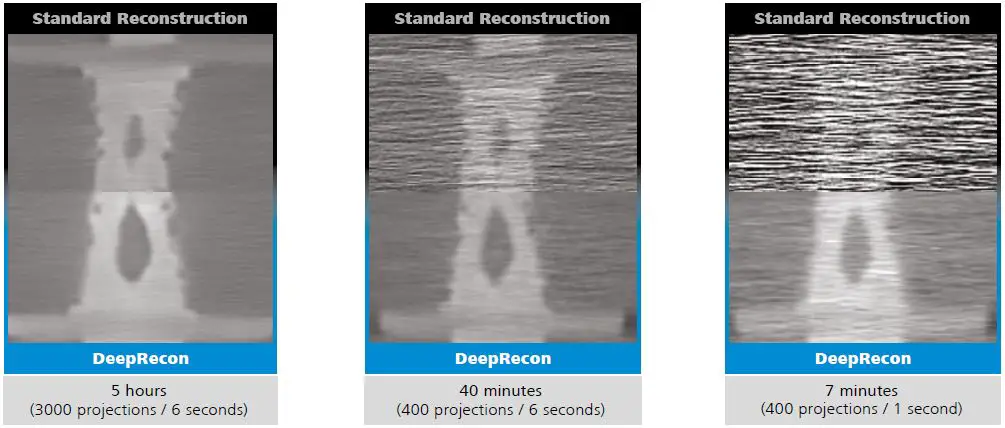
Tremendous speed advantages can be realized for larger features, and even fine features can be analyzed with a good ratio of image quality to speed.
About ZEISS Xradia X-ray Imaging Solutions
ZEISS provides innovative X-ray hardware and software to meet the following challenges:
- Achieving the right ratio of resolution versus throughput (application and sample dependent)
- Achieving scan speeds as required for the full workflow (application and sample dependent)
- Visualizing submicron defects in large structures without the need for sample preparation and with a large FOV (i.e. to enable visualization of 100 nm diameter cracks within an intact 100 μm C4 bu mp)
- Visualizing defects and structures as interconnect pitch drops below 10 μm
- Mitigating beam hardening and other X-ray artifacts
- Minimizing dose (due to device radiation concerns)
ZEISS continuously develops new solutions to solve these challenges for semiconductor package analysis and FA applications. ZEISS offers unprecedented system extendibility with field conversion options and various u pgrades like DeepRecon to protect your investment.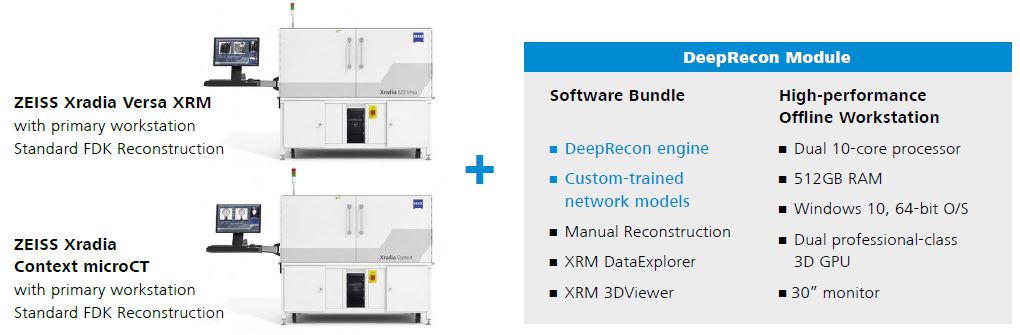
ZEISS Process Control Solutions (PCS)
Carl Zeiss SMT, Inc.
4385 Hopyard Road
Pleasanton, CA 94588
USA
www.zeiss.com/pcs
[email protected]
ZEISS DeepRecon Faster 3D X-ray imaging throughput and superior Instruction Manual – Optimized PDF
ZEISS DeepRecon Faster 3D X-ray imaging throughput and superior Instruction Manual – Original PDF
References
]]>
ZEISS OptiRecon
Improve 3D X-ray image quality and increase scan speed by 2X
for semiconductor packages
The new ZEISS OptiRecon option for ZEISS Xradia Versa X-ray microscopes (XRM) and Xradia Context microCT enables significantly faster 3D X-ray image acquisition at any energy setting through an image reconstruction algorithm known as iterative reconstruction.
In addition to speeding up analysis, OptiRecon also can provide better image quality at standard scan speeds. It is well-suited for failure analysis (FA) and development applications across a wide variety of semiconductor packages.
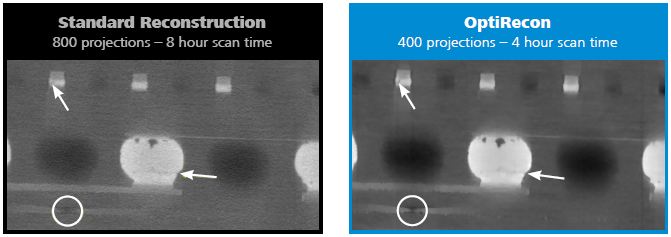
Up to 2X Faster Scans at Similar Image Quality
OptiRecon produces high-quality images having high contrast-to-noise ratios. It allows for fewer projections than the conventional reconstruction method known as Feldkamp-Davis-Kress (FDK), while achieving similar quality as FDK reconstructed images. The reduced number of projections enables significantly faster data collection, even when using low kV settings to maximize image contrast. The ability to see fine featu res and defects is retained across a broad range of samples and defect types.
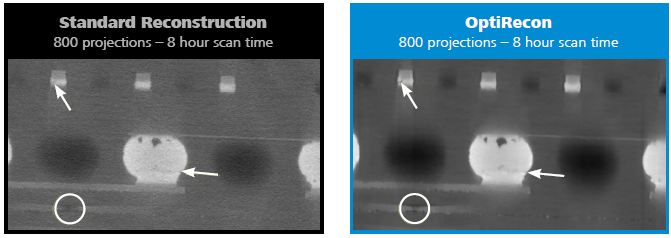
Improved Image Quality
OptiRecon can improve image quality of full-projection datasets. Identifying small defects in a >1 mm volume of data can be challenging and requires sharp analytical eyes. High image contrast, high spatial resolution and high signal-to-noise ratios all drive the imaging quality. When applied to full-projection datasets, OptiRecon reduces noise resulting in images with both high contrast-to-noise and high signal-to-noise ratios. This improves defect visualization, reduces eye fatigue for the analyst, and increases FA success rates.
Fast and Efficient
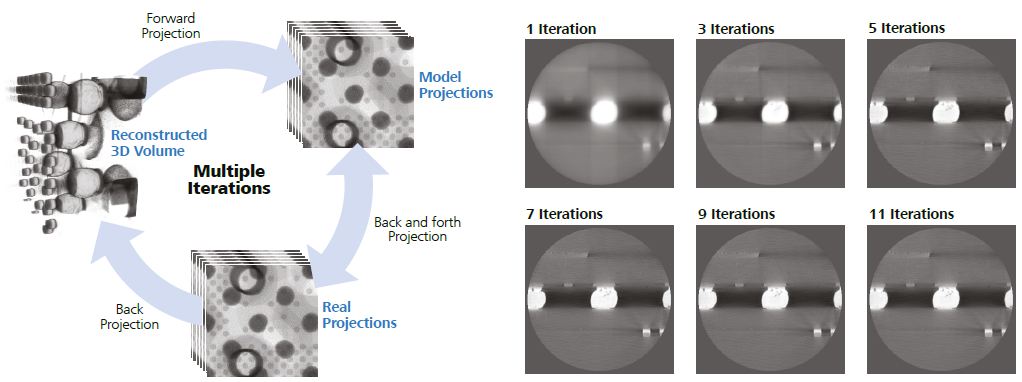
Iterative reconstruction is significantly more computationally intensive than the standard filtered-back projection technique and can require very long reconstruction times.
OptiRecon features a proprietary, efficient implementation that can achieve reconstruction of a standard dataset of 1024 x 1024 x 1024 voxels from 400 projections in about 5 minutes. It includes an advanced high-performance offline workstation and easy-to-use interface to optimize reconstruction parameters.
User-friendly
Iterative reconstruction as implemented by other manufacturers requires a skilled user with expertise to fine-tu ne the process parameters for each application. The ZEISS workflow-based OptiRecon user interface has easy-to-use parameter tuning that does not require expertise in tomographic reconstruction techniques.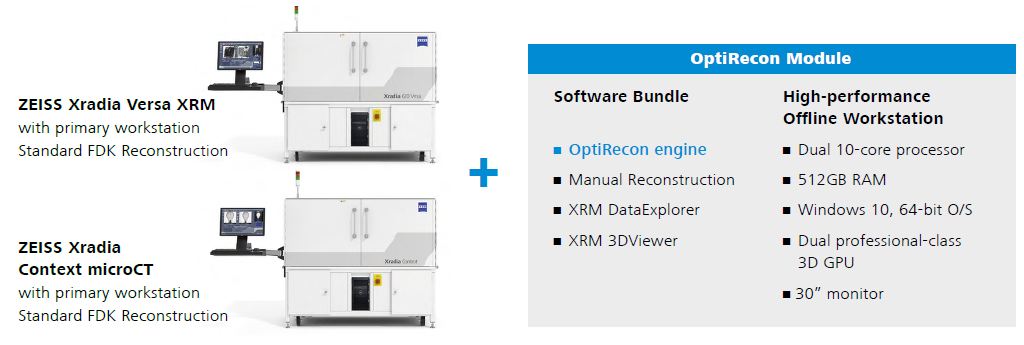
Set up is accomplished in 4 easy steps:
- Select dataset
- Perform standard parameter optimization: center shift, beam hardening
- Perform OptiRecon parameter optimization with visual feedback: edge preserving and smoothing (noise reduction)
- Reconstruct
OptiRecon is offered via the unique Advanced Reconstruction Toolbox for ZEISS Xradia 3D X-ray systems. It is compatible with ZEISS Xradia 410, 500- and 600-series Versa 3D XRM and Xradia Context microCT. ZEISS offers unprecedented system extendibility with field conversion options and various u pgrades like OptiRecon to protect your investment.
ZEISS Process Control Solutions (PCS)
Carl Zeiss SMT, Inc. 4385 Hopyard Road Pleasanton, CA 94588 USA
www.zeiss.com/pcs
[email protected]
ZEISS OptiRecon option for ZEISS Xradia Versa X-ray Microscopes Instruction Manual – Optimized PDF
ZEISS OptiRecon option for ZEISS Xradia Versa X-ray Microscopes Instruction Manual – Original PDF
References
]]>
This document provides updated guidance from ZEISS on how to treat the Humphrey® perimeter to promote patient safety during visual field examinations and guidance is provided on how to clean the bowl, should the clinic determine that such cleaning is desired.
Between each patient use, all patient and technician interface surfaces excluding the bowl, may be wiped down using isopropyl alcohol. These include the eyepatch, patient chinrest, headrest, patient response button, trial lens holder and trial lenses, as well as all technician user interfaces.
If there is a desire to clean the bowl of the HFA, the bowl surface may be treated by spraying it with a 70% isopropyl alcohol (IPA) solution. The following are step-by-step instructions on the recommended procedure for sanitization of the HFA between patient tests. This procedure is applicable to all HFA models including HFA3, HFA II-i, and HFA II.
In order to reduce the possibility that repeated misting of IPA70 could affect sensitive optical and electromechanical components in the HFA bowl area, we recommend using simple paper coverings during the misting process as described in this procedure.
Preparation Steps
Step 1: Gather the appropriate materials for cleaning
- 70% Isopropyl alcohol (IPA70)
- Fine misting sprayer – see recommendations in References
- Printer paper – size: US Letter, A4, or similar
- Soft cloth, lens tissue, or cotton swab
Step 2: Prepare cleaning materials
- Prepare a 70% IPA solution using 7 parts IPA (100%) and 3 parts distilled water. Alternatively, commercially available 70% IPA is also acceptable.
Fill the fine misting sprayer with IPA70 solution. Perform a test spray away from the instrument to ensure that the sprayer produces a gentle, fine mist.

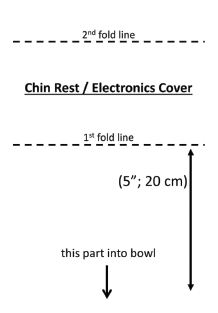
Step 3: Prepare Paper Coverings
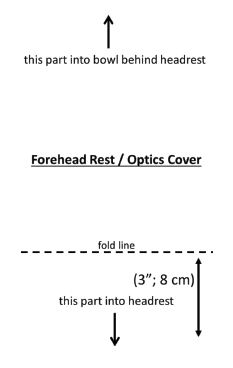
Chin rest paper cover: Fold the paper approximately 5” (20 cm) from the edge, then fold the other edge in half. Forehead-optics paper cover: Fold the paper approximately 3” (8 cm) fromthe edge.
Forehead-optics paper cover: Fold the paper approximately 3” (8 cm) fromthe edge.

HFA Sanitization Procedure
- The HFA instrument should remain powered ON during the sanitization procedure and between patients.
- The normal airflow through the bowl will help to circulate the IPA70 mist within the bowl and in general, circulate air through the bowl.
- If in your judgment the bowl appears dusty, follow the HFA Instructions for Use, which describes that occasional wiping with a soft cloth and isopropyl alcohol may be performed.
Step 1
Between patients, wipe the forehead rest, chin rest, patient response button, trial lens assembly and lenses, operator interfaces and exterior panels near patient area in accordance with CDC or local public health guidelines and your own infection control procedures (alcohol wipes or similar).
Step 2
Lower the trial lens holder into the area behind the chin rest.
Step 3
Place the chin rest paper cover over the chin rest so it covers the opening behind the chin rest in order to protect electronics from getting wet.
Step 4
Insert the short side of the forehead-optics paper cover into the gap between the forehead rest and the instrument.
Step 5
Hold the IPA70 mist spray bottle in one hand. With your other hand, roll the forehead-optics paper cover in and hold at the free edge to cover the optics area behind the head rest.
Step 6
Hold the misting sprayer in the bowl maintaining a distance of about 15 cm from the bowl surface. Spray in a sweeping motion so that the entire bowl surface develops a wet appearance, but stop before droplets form.
Step 7
Blot dry any drips or puddles in the bowl with a clean soft cloth or lens tissue. Avoid wiping or rubbing the bowl surface.
Step 8
Wait until the IPA70 dries (approximately 5 – 10 minutes).
Step 9
Remove paper coverings. Raise trial lens holder if needed for next test.
Step 10
The HFA is now ready for testing the next patient.
References and Material sources
Note: These are suggestions of materials sources, not a requirement for specific models.
Fine Misting Sprayers:
- https://www.amazon.com/Continuous-Misting-Sprayers-cleaning-Planting
- https://www.amazon.com/Beautify-Beauties-Flairosol-Empty-Bottle
- https://www.walmart.com/ip/Hairdressing-Spray-Bottle
- https://www.amazon.com/Essential-Refillable-Atomiser-Perfume-Cleaning
For additional resources on COVID-19, please visit our MED Support now website,
www.zeiss.com/med-support-now
Paper cover templates:
Print the next two pages on separate pieces of paper to use as templates for your Chin Rest and Forehead Rest covers.
Zeiss Humphrey Perimeter [HFA3, HFA II-i, HFA II] User Manual – Optimized PDF
Zeiss Humphrey Perimeter [HFA3, HFA II-i, HFA II] User Manual – Original PDF
References
]]>This guide is an overview of scan acquisition for scans available* with CIRRUS HD-OCT software version 8.0. See the CIRRUS HD-OCT Instructions for Use for safe and effective operation.
1. Find the pupil and focus the image in the iris viewport.
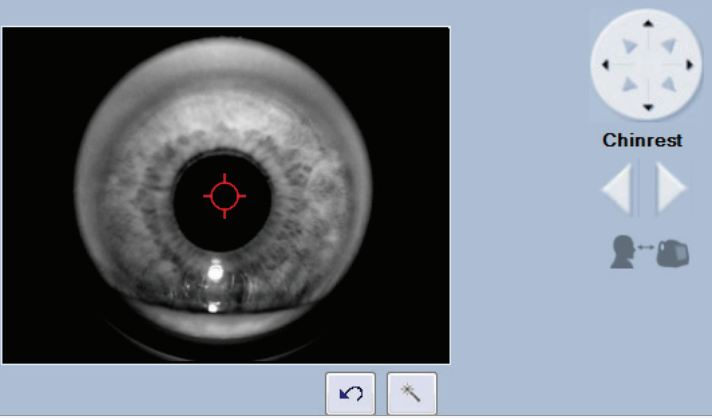
Adjust table height.
Place patient’s chin in the left chin cup (marked blue) to scan the right eye or the right chin cup (marked white) to scan the left eye. Patient’s forehead should make contact with the headrest. Adjust the chinrest height to align the canthus marker with the patient’s eye.
Adjust the patient position to find the iris and pupil. Use the chinrest controls or click on the pupil in the iris viewport. Instruct the patient to move with the chinrest. The patient should not hold on to instrument. Click within the center of the pupil for final alignment.
Use  to obtain a clear focus on the iris. This helps the system set the position for the OCT scan.
to obtain a clear focus on the iris. This helps the system set the position for the OCT scan.
Advanced Tips
- Click on the icon to adjust the brightness, contrast, and illumination. Lowering the illumination may increase pupil size.
- The mouse scroll wheel can be used to make fine changes to the iris image in/out adjustment.
- During subsequent steps, monitor: 1) the patient’s head to ensure they maintain contact with the headrest and, 2) the position of the red scan
circle in the pupil to ensure it remains within the pupil.
2. Make adjustments for optimal fundus and B-scan images.
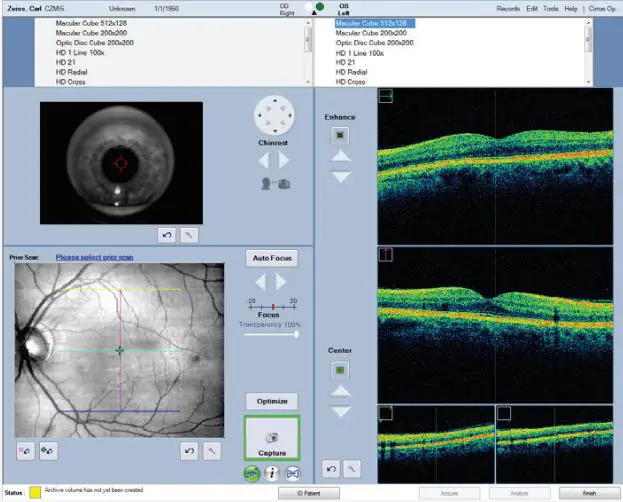
Click on Auto Focus. Instruct patient to move with the chinrest, fixate on the target and to not blink while this function runs. Adjust manually if necessary. Proper focus can increase the signal for the OCT scans and improve ability to track.
Click on Optimize to center and enhance the B-scan images. To sharpen the fundus image, mouse over the fundus image and click on the wand that appears in the upper right corner to perform auto B/C.
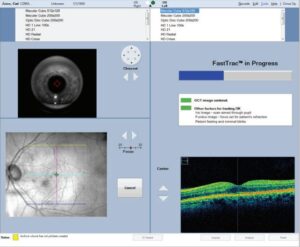
Performing a scan with FastTrac™
- When the border around the Capture button is green, you are ready to acquire the scan
with FastTrac. If the border is red, further actions can be taken: - Center the scan with the Center controls or hold Shift and roll the mouse wheel.
- Click Auto Focus or manually adjust focus to sharpen fundus image quality.
- Change the prior scan or disable Track to Prior button
 for this scan.
for this scan. - You can turn off tracking by clicking the FastTrac button
 .
.
Advanced Tips
- The B-scan images should show a range of colors. Faint green B-scans indicate that the signal is low.
- To modify brightness or contrast for either the B-scans or fundus images, click near the image of interest and adjust the controls.
Note: The setting changes made for the B-scans here will persist for future scans. - If the OCT image appears inverted, click the Center up/down buttons several times until the image flips and is centered it in the window.
- Center the B-scan images and ensure all B-scan images are not too high or too low. This could result in missing data in the scan.
- For highly myopic patients it may be necessary to click the Auto Focus button a second time.
- Moving the scan in the pupil in the iris viewport can help if: 1) there are media opacities, 2) the OCT B-scans appear tilted.
- Instead of using Auto Focus, enter spherical equivalent information on the patient demographic page for CIRRUS to pre-focus to this value.
- When tracking on the macula with patients with tilted retinas, you can improve success using tracking by turning off the system’s center
position monitoring. Click on the wand next to the bottom B-scan, then in the dialog box, uncheck Monitor Z position.
3. Capture the fundus image and high-density scan
When the fundus image and B-scans are optimized, tell the patient to blink once or twice.
Then tell the patient to open wide and maintain focus on the center of the green fixation
target.
Click Capture.
Avoid a patient blink right at the moment you intend to click Capture.
If tracking is on, you can tell the patient to blink naturally during the scan.
If tracking is off, remind the patient to avoid blinking and to focus on the target until the capture is completed.
FastTrac Scan in Progress Screen. When FastTrac is interrupted, the progress bars turn red and processing stops. Click Cancel to return to the Acquire Screen to make adjustments to center the scan, focus the fundus or iris images, or turn off FastTrac for a non-tracked scan.
4. Review the captured scan, then save or try again
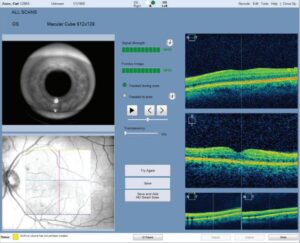
On the Review screen, evaluate the B-scan quality and the Signal Strength (6 or greater). Check that the OCT B-scans are approximately centered in the windows without missing data.
If scan quality, position, or eye movements are unacceptable, click Try Again to retake the scan.
Adjust brightness and contrast by right clicking on the fundus or OCT image. The B/C values set on the review screen are saved and used for analysis for this scan only.
Click Save.
If you perform another scan on the same eye, the patient can stay positioned. Otherwise, the patient should sit back.
Add a Smart HD Scan
With the Smart HD scan workflow, you can automatically track HD scans to the fovea. Acquire a Macular Cube 512×128 or Macular Cube 200×200 scan. Auto FoveaFinder™ automatically locates the fovea. Alternately, target a specific region of interest with a Smart HD scan by moving the slice navigators.
On the Review screen, click the Save and Add Smart HD Scan button. The Macular Cube scan is automatically saved and an HD scan is initiated and tracked to the fovea location.
On the Acquire screen, click Capture, and then on the Review screen, click Save.
Note: To make adjustments to line spacing, rotation, or length of the Smart HD scan, first turn off Track to Prior, make adjustments, and then turn Track to Prior back on before clicking Capture.
Note: The last Smart HD scan used for the Smart HD scan workflow becomes the default scan.
Advanced Tips
- Examine the high definition en face scan closely for any subtle eye movement. Also slide the Transparency control back and forth to compare the images.
If noteworthy movement is detected, click Try Again. - If the next scan will be on the other eye, choose the scan pattern for that eye before the patient returns their head to the appropriate chin cup and headrest. This can help avoid
contact with the patient’s nose. - During a scan with FastTrac, individual B-scans in a cube may be acquired at slightly different positions, resulting in horizontal lines or bands on the fundus image. If there are no saccades, a scan with bands in the OCT fundus should be acceptable for analysis.
- Smart HD Scans automatically find the fovea based on the Macular Cube scan information.
You can also use the Macular Cube to target a specific feature for a Smart HD Scan.
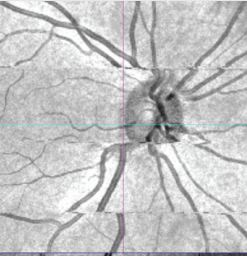
Example: Saccades (vessel mismatch)
Example: Banding (no vessel mismatch)
Zeiss 5000 CIRRUS HD-OCT Scan Acquisition User Manual – Optimized PDF
Zeiss 5000 CIRRUS HD-OCT Scan Acquisition User Manual – Original PDF
References
]]>
How do I serial transfer data from an HFA II or HFA II-i to an HFA3?
ZEISS Quick Help: Humphrey ® Field Analyzer II, II-i, and 3 (HFA II, HFA II-i and HFA3)
Data can be transferred from an HFA II or an HFA II-i to an HFA3. However, data cannot be transferred from an HFA3 back to an HFA II model.
Start the transfer by making a pre set-up check
- Verify that the HFA II is at software Rev. 14.0 or greater and/or that the HFA II-i is at Rev. 3.5 or greater. This can be checked by looking at the upper left corner of your instrument screen.
- Check the Database Status to determine the approximate time to complete the transfer. From the Main Menu, go to File Functions, and then Database Status. Record the number of Hard Drive Tests and divide by 800. This gives you the approximate number of hours to complete the transfer.
- Connect your instruments. Transferring data between the two machines requires a custom serial data cable connection. You will need a serial cable connected to a USB cable. The cables are included in the accessory kit of the HFA3. If you cannot locate your cables, replacement cables can be ordered by calling ZEISS and asking for a custom serial cable for a Humphrey Field Analyzer (PN 2660021151011) and a USB cable (PN 2660021155206).
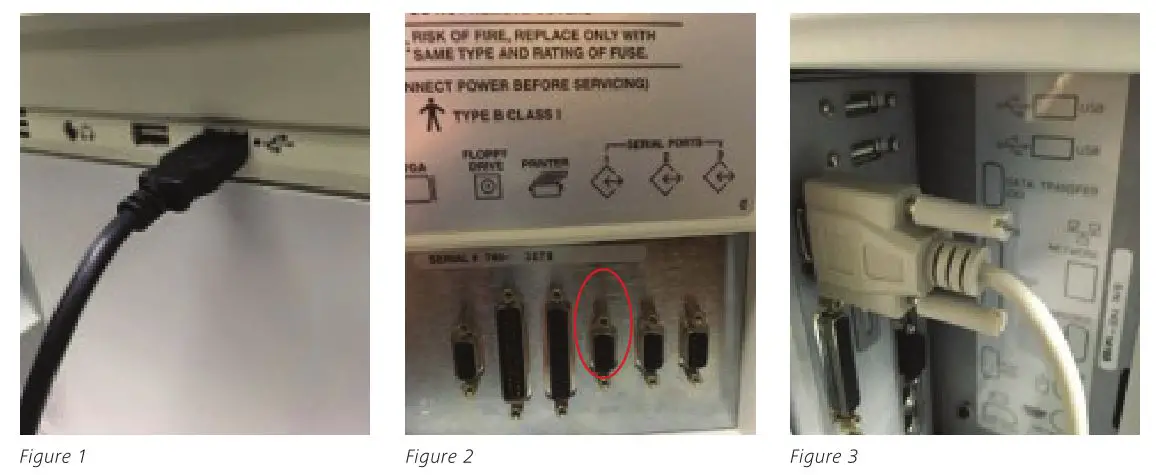
- Connect the USB end of the cable to one of the front USB ports on the HFA3 (Figure 1). Connect the serial end of the cable to the HFA II or II-i. If you have an HFA II, the ports are located at the back of the instrument. The cable must connect at serial port number one, third from the right (Figure 2). If you have an HFA II-i, the cable connection is located behind the hinged panel at the back of the instrument (Figure 3).
Set up the Data Transfer on the HFA3:
- From the Main Menu, select Settings, select Advanced Settings, select HFA Data Transfer.
- Follow the detailed instructions on the screen.
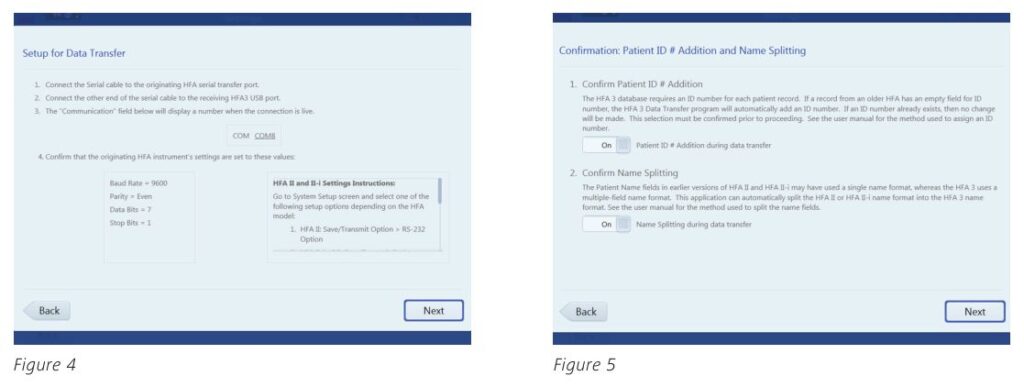
- Select Next once the two instruments are connected (Figure 4).
- In the next screen (Figure 5), choose ON to add a patient ID number during data transfer. This feature is required for data import. A unique 29-character Patient ID, if currently missing, will be automatically created for the patient from the patient’s name and date of birth. If an ID number exists, it will not be altered.
- Select ON to add name splitting during data transfer. HFA II and HFA II-i (software versions before 5.0) use a one name field for patient records. To generate a report using patient data on the HFA3, you must change the patient record to include a separate first and last name.
- Select Next. The HFA Data Transfer screen will then appear (Figure 6).
- Select Transfer Instructions and choose either the HFA II or HFA II-i tab (Figure 7) to display specific transfer instructions for your model. Go to the proper HFA II device and follow the steps.
Note: On the HFA II or HFA II-i, when you are ready to choose the tests you want to transfer, at the keyboard select the Enter Key and then Select All to transfer all tests at one time.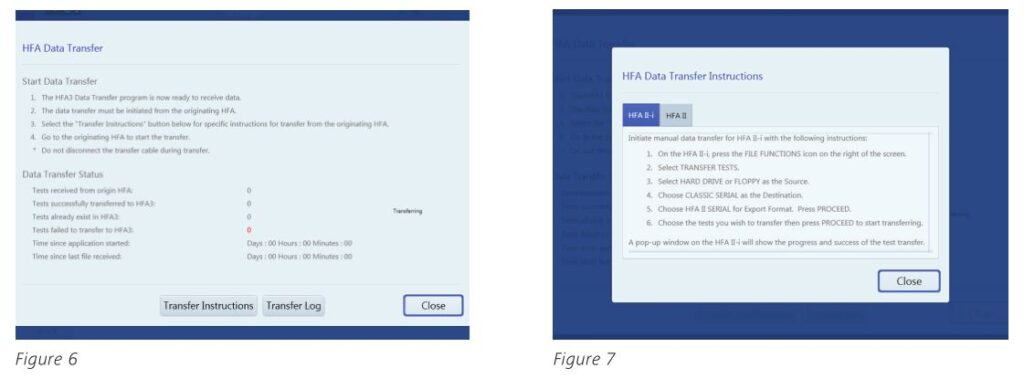
- Back on the HFA3, select Close to return to the previous screen to monitor the Data Transfer Status on the HFA3. Once you’ve started the transfer, it’s very important to look at the HFA3 screen to ensure that it’s actually receiving tests, and that the number of tests transferred is increasing.
- At any time, you can select Transfer Log to view a summary of the data transfer. Expect that 10 percent, or less, of the total tests will not transfer, generally because they are invalid or incomplete.
Tests that will not be transferred:
- Fast Threshold tests of Master files
- Compared, Averaged or Merged exams
- Tests without birthdates or with invalid birthdates
- Tests without patient names
- Tests with invalid test dates
- Tests without LEFT or RIGHT denoted in eye field
- Tests that have invalid (x,y) coordinates for test points
Refer to the Humphrey Field Analyzer user manual Instructions for Use for safe and effective operation of the instrument.

 Carl Zeiss Meditec Inc.
Carl Zeiss Meditec Inc.
5160 Hacienda Drive
Dublin, CA 94568
USA
www.zeiss.com/med
 Carl Zeiss Meditec AG
Carl Zeiss Meditec AG
Goeschwitzer Str. 51-52
07745 Jena
Germany
www.zeiss.com/med
SER.8188 Printed in the USA CZ-09/2016
The contents of this reference guide may differ from the current status of the product in your country. Please contact your regional representative for more information. Subject to change in design and scope of delivery and as a result of ongoing technical development. Humphrey and HFA are either trademarks or registered trademarks of Carl Zeiss Meditec, Inc. in the United States and/or other countries. © 2016 Carl Zeiss Meditec, Inc. All copyrights reserved.
Zeiss Humphrey Field Analyzer [HFA II, or HFA II-i, HFA3] User Manual – Optimized PDF
Zeiss Humphrey Field Analyzer [HFA II, or HFA II-i, HFA3] User Manual – Original PDF