
![]()
PATIENT EDUCATION GUIDE
![]()
Need help or have questions? Contact Customer Service Toll Free at 1.877.593.6421 or visit myheartmonitor.com for online support.
CardioNet, LifeWatch and BioTel Heart are trademarks of BioTelemetry, Inc. BioTelemetry reserves the right to change specifications at any time without notice.
Before you Begin
About our Service
Your physician has prescribed ePatch™ for you. ePatch continuously records and stores heartbeats that are analyzed by certified cardiac technicians at BioTel Heart®. Clinical reports are made available to your healthcare provider at the end of service.
To get started, review the important information in this guide or visit myheartmonitor.com.
If you have any questions, please contact us:
Customer Service: 1-877-593-6421 (toll-free)
email: [email protected]
Hours: Mon-Fri 8am – 8:30pm EST; Sat 8am – 4:30pm EST
Kit Contents
1 2 3

4 5 6

7
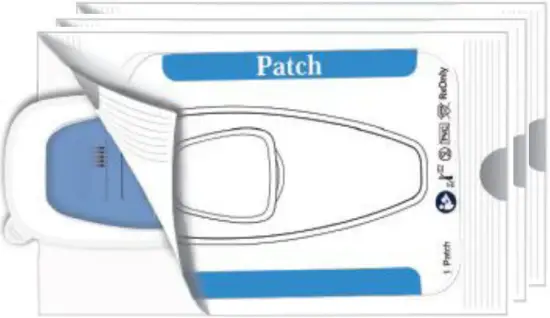
- Sensor
- Patch Pouches
- Scrub Pad
- Patient Education Guide
- ePatch kit with return label attached to the box
SAVE THE BOX! - Diary
- Patch Template
What to Expect During Service
Contacting You
Before, during or after your service, we may contact you for any of the following reasons:
- Confirm insurance information
- Assist with starting service
- Confirm a break in service
- Troubleshooting
- On behalf of your physician
(please note, we will not contact you regarding heart-related findings, unless specifically instructed by your physician)
 Billing for Service
Billing for Service
Your insurance company will send you an Explanation of Benefits (EOB). An EOB from your insurance carrier is NOT a bill.
You will be responsible for any out-of-pocket cost associated with deductibles, co-insurances, etc. If there is a balance due, you will receive a statement from BioTel Heart for your portion. If you have any questions regarding the balance due, please refer to your statement for contact information.
 Prompt Return of All Equipment
Prompt Return of All Equipment
The device and kit components enclosed are the property of BioTel Heart and must be returned immediately upon completion of service. Failure to return may result in delayed delivery of the final test results and a bill for the cost of the device. Device Return instructions are located in this guide. Please refer to the Table of Contents for page number.
Getting Started
Quick Start Instructions
Step 1
SHAVE (If needed), then WASH and DRY area shown in diagram thoroughly.
Once skin is dry, SCRUB area with the SCRUB PAD for one minute. DO NOT apply lotions or oils.
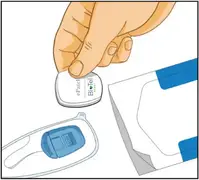
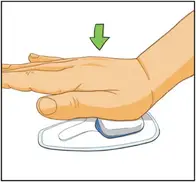
Remove a patch from the patch pouch. Place sensor into patch and PRESS down firmly to snap it in place.
Step 2
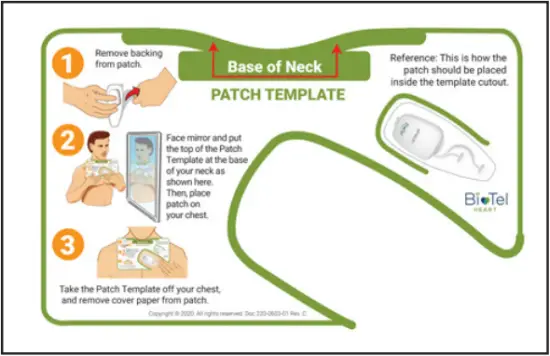
Locate the Patch Placement Template in the kit and follow its instructions for use.
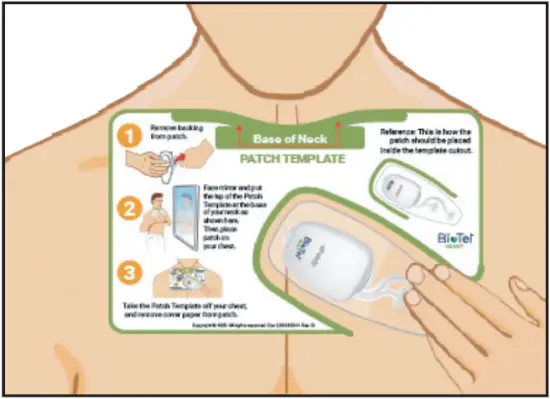
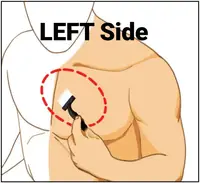
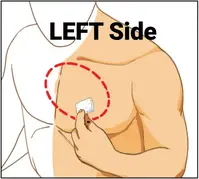
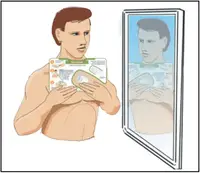
REMOVE CLEAR BACKING and apply the patch to your chest using the template as a guide as shown. Use a mirror for guidance. Remove template when finished.
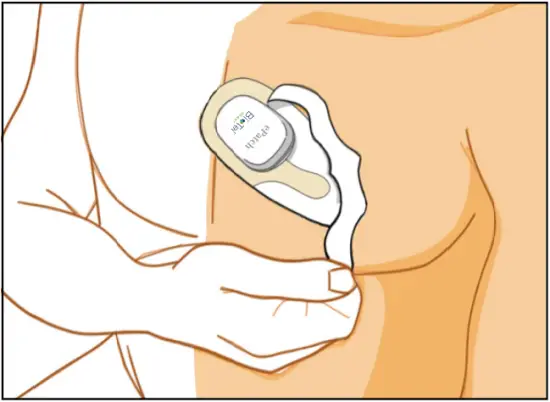
Press the patch firmly against your skin then REMOVE TOP WHITE PAPER.
IMPORTANT: DO NOT THROW THE BOX AWAY. YOU WILL NEED TO USE IT TO RETURN THE EQUIPMENT AND SUPPLIES.
Good to Know
Record Symptoms

- Whenever you feel a heart-related symptom, double tap the middle of the sensor to record the symptom. When the sensor has registered the symptom, the status indicator will show a constant green light for one second.
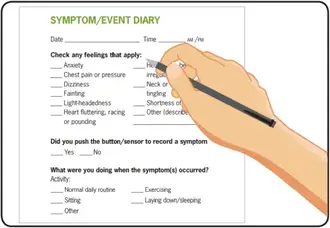
- Make sure to write that symptom and how you are feeling in the diary.
- Locate the diary in your kit and fill in your name, address, physician’s name, and the start date. After your monitoring period has ended, fill in the date you removed ePatch.
- Do not forget to include the date and time of each symptom.
Removing the Patch
Step 1
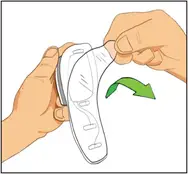
How to REMOVE the SENSOR from the PATCH
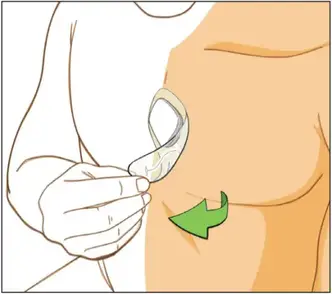
Remove the patch by pulling the clear adhesive away from your body.
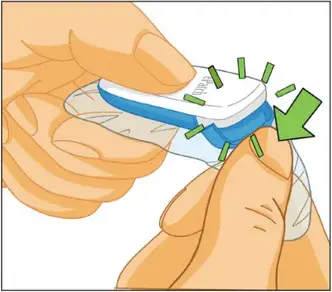
Apply downward pressure on the tab to snap/break it off. This will require some force.
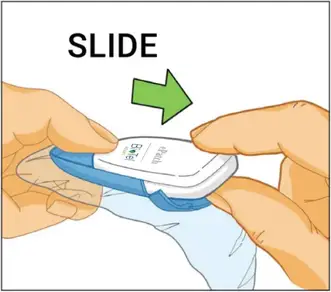
Hold the sensor as shown and slide the sensor forward to remove it from the patch.
Discard the used patch,
Step 2
How to apply a NEW PATCH
Additional patches are provided in the kit if you plan to wear ePatch for a longer duration, or if you are experiencing discomfort. Please refer to the Getting Started section of this guide to set up and apply a new patch.
Returning ePatch
Step 1
" sizes="(max-width: 287px) 100vw, 287px" alt="ePatch PBT - Returning ePatch 1" width="287" height="152" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-1-550x291.png 550w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-1.png 667w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-1-550x291.png" />
Important: Do not throw the box away. You will need to use it to return the equipment and supplies.
Step 2
" sizes="(max-width: 190px) 100vw, 190px" alt="ePatch PBT - Returning ePatch 2" width="190" height="157" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-2-550x457.png 550w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-2.png 705w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-2-550x457.png" />
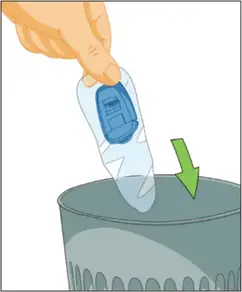
When you are ready to return ePatch, pack up the sensor, unused patch pouches, diary and any other supplies, and place into the kit.
Step 3
" sizes="(max-width: 228px) 100vw, 228px" alt="ePatch PBT - Returning ePatch 3" width="228" height="143" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-3-550x344.png 550w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-3.png 625w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Returning-ePatch-3-550x344.png" />
Remove the protective strip to expose the adhesive. Seal the kit shut. Return the pre-paid sealed kit back to BioTel Heart via UPS. You can find the nearest available location by going to www.ups.com/dropoff. There is no cost to you to mail back the equipment. If you are unable to bring ePatch to a UPS drop off location, please call 1-877-593-6421 for instructions on how to schedule a pick up. Remember to mention that you have a UPS pre-paid label.
Showering Instructions
" sizes="(max-width: 112px) 100vw, 112px" alt="ePatch PBT - Showering Instructions 1" width="112" height="112" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-1.png 448w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-1-150x150.png 150w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-1.png" /> Shower or exercise as normal while wearing ePatch.
" sizes="(max-width: 112px) 100vw, 112px" alt="ePatch PBT - Showering Instructions 2" width="112" height="112" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-2.png 447w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-2-150x150.png 150w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Showering-Instructions-2.png" />
Do NOT swim or bathe.
Patch is water-resistant, not waterproof.
Important Information
" sizes="(max-width: 278px) 100vw, 278px" alt="ePatch PBT - Important Information" width="278" height="178" data-ezsrcset="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Important-Information-550x352.png 550w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Important-Information-768x491.png 768w,https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Important-Information.png 797w" data-ezsrc="https://manuals.plus/wp-content/uploads/2022/03/ePatch-PBT-Important-Information-550x352.png" />
- Continue to wear ePatch for the duration prescribed by your physician.
- Mild itching or irritation underneath the patch area may occur, and is usually temporary. If more significant itching or irritation develop or persists, contact Customer Service at 1-877-593-6421.
- Write down any symptoms as they occur in your diary.
For assistance, please call Customer Service at 1-877-593-6421
ePatch™ ADDENDUM TO THE PATIENT EDUCATION GUIDE
Indications for use
ePatch is indicated for use on patients who may be asymptomatic or who may suffer from transient symptoms such as palpitations, shortness of breath, dizziness, light headedness, presyncope, syncope, fatigue, chest pain and/or anxiety.
ePatch is intended for use by adolescents 18-21 and adults.
Contraindications
The sensor is not intended for use on:
• Patients with implanted pacemakers.
The compatible ECG patch is not intended for use in the following cases:
• The compatible ECG patch is not intended for use on patients with known allergies to adhesive materials or hydrogel.
• The compatible ECG patch should not be placed on broken, damaged, or irritated skin.
RX only
Caution: Federal law restricts this device to sale by or on the order of a physician.
Precautions
Avoid contact with the eyes or mucus membranes of gels, alcohol, acetone, or any substance used in the placement or removal of the patch. This can damage the eyes or mucus membranes of the patient.
Do not use an obviously broken sensor. This can cause electric discharge or decrease the quality of the acquired signals.
Do not touch the terminals at the backside of the sensor or let them touch other conductive parts or earth. This may damage the sensor.
Minimize the number of devices connected to the patient. Otherwise, there is a risk of accumulation of leakage current.
Store and use the sensor within temperature, pressure, and humidity ranges specified in Section 8.1.4. Avoid exposing any part of the sensor to heat sources, heat radiators and fireplaces, direct exposure to sunlight, nebulizers, or electrical steam kettles. Temperature changes cause condensation and moisture that can lead to malfunction of the sensor. Before using the sensor, allow the sensor to acclimate to ambient temperature. For reference, if the temperature difference between the sensor and the environment is above 10ºC, a 20 minutes wait time in an intermediate temperature is recommended.
The sensor is only splash proof (Protection level IP24) when it is correctly connected to a compatible patch. Otherwise, it is not splash proof. This implies that the sensor should not be exposed to any kind of liquid when it is not connected to a compatible patch. Even when the sensor is correctly connected to a compatible patch, it should never be exposed to a direct jet of water or any other liquid material. This might cause electrical short circuiting of the sensor.
Do not expose the internal parts of the sensor, the provided sensor charger adapter, or the provided USB power adapter to any liquids. Do not submerge the sensor, the provided sensor charger adapter or the USB power adapter in any liquid. This may cause electric short circuiting or electrical discharge.
Mobile phones, transmitters, and similar equipment generating radio frequency (RF) emissions should not be used or placed next to the sensor during recordings. This can affect the sensor. Follow the recommendations regarding the separation distance specified in the manufacturer’s declaration for EMC in this Instruction Manual, see Annex 1.
Warnings
Do not use the sensor in an X-ray, computed tomography (CT), or magnetic resonance imaging (MRI) environment. This may affect the scanning results, it can lead to malfunction of the sensor, and it may result in injuries to the patient.
Do not attempt to open, adjust, or modify the sensor, the provided Micro USB cable, or the provided USB power adapter. This can lead to electrocution, burns, and malfunction.
Always use the sensor together with compatible accessories (patches, Micro USB cable, and USB power adaptor) that are supplied by the manufacturer. Use of other equipment may result in increased emissions or decreased immunity of the sensor and can cause damage to the device or decrease the quality of the acquired signals. Use of other equipment or un- approved patches might also lead to skin irritations, allergy, electrical shock, and malfunction of the sensor. Use of other chargers may damage the device and/or the accessories.
Do not connect the sensor to other equipment than specified in this Instruction Manual. This can lead to previously unidentified risks.
Keep the sensor, the patches, the provided Micro USB cable, and the USB power adapter out of reach of children, pests, and pets. There is a danger of strangulation if the provided Micro USB Cable is misused. There is a danger of choking if the sensor and/or the accessories are swallowed.
Do not use a defibrillator on a patient wearing the sensor. The sensor is not protected against defibrillation shocks. Use of a defibrillator can lead to injuries to the patient and malfunction of the sensor. Remove patch and sensor prior to defibrillation.
Specifications
Device
Device classification (EN 60601-1): Class: Internally Powered, Type BF applied parts, not protected against defibrillator, no functional earth terminal
Data acquisition: 1, 2, or 3 channels ECG, Event Triggera
Recording time: Default of 5 days (the recording time is configurable by manufacturer)
Sampling rate: 128, 256, 512, or 1024 Hza
Resolution: 12 bit or 16 bit, depending on customer presence
Frequency response: 0.05 Hz High Pass
Input range ECG Channels: 180 mVpv (Peak-to-Valley) CMRR (common mode rejection ratio): >80 dB
Input impedance: 10 MΩ
Connections: 1 ePatch™ 2.0 Specific 8-Terminals Connector for connection to a compatible patch
Storage medium: 2 GB internal storage
Maximum data file size: 2 GB EFS-file (ePatch™ 2.0 File System)
Expected service life: Minimum 500 lifecycles or minimum two years (after which the battery capacity, or available service time from a full charge, of the sensor may be reduced)
a The number of recorded ECG channels and the sampling frequency depends on the configuration of your sensor. Note that not all combinations of channels and sampling frequencies are possible.
b The default recording time for a configuration with two ECG channels and a sampling frequency of 256Hz is max. five days but other configurations are possible, if requested from manufacturer.
The maximum possible recording time is increased when the number of recorded ECG channels and/or the sampling frequency is decreased. Likewise, the maximum possible recording time is de creased when the number of recorded ECG channels and/or the sampling frequency is increased. See annex II for recording times for various configurations. Note that the recording time of your sensor might be configured to be less than the maximum possible recording time.
Battery
The sensor is powered by an integrated battery with the following specifications:
Type: Rechargeable lithium-ion polymer battery
Battery capacity: Typical 500 mAh
Nominal voltage: 3.7 V
Charging voltage: 4.2 V
Battery life: Minimum 500 recharges
Charger: USB 5.0 VDC, 250 mA
The battery is not replaceable. Charging of the sensor should only be performed by use of the provided sensor charger adapter with the USB power adapter or a computer via the provided sensor charger adapter. Use of other charging devices may damage the device and/or the accessories.
CAUTION
Always keep the battery charged when sensor is not in use. For periods of extended storage, fully charge the device and fully recharge once every 12 months. Not following this guideline may reduce total battery capacity and increase wear.
Measure and weight
Sensor
Measures (W x H x D): 40 x 49 x 12 mm
Weight: 20 g
Environment
Enclosure protection degree: IP24 (when the sensor is connected to a compatible patch/ electrode)
Operating conditions
Temperature: +5°C to +40°C
Pressure: 700 - 1060 hPa
Relative humidity: 15% – 90% (non-condensation)
Transport and Storage conditions (including between uses)
Temperature: 25°C to +50°C
+5°C to +35°C at relative humidity up to 90%, non-condensing
>35°C to 70°C at a water vapor pressure up to 50 hPa
Relative humidity: 15% – 90% (non-condensation)
Shelf life: Non-perishable, battery charge level to be maintained.
Exceeding the recommended operating, storage, and transportation conditions may result in reduction of the performance of the sensor and/or accessories
Environment (Patch)
Enclosure protection degree: IP24 (when the sensor is connected to a compatible Patch)
Operating conditions: Temperature: +5°C to +40°C
Pressure: 700 - 1060 hPa
Relative humidity: 15% – 93% (non-condensation)
Storage conditions (including between uses):
Temperature: 5°C to +27°C
Relative humidity: Up to 93% (non-condensation)
Transportation conditions
Temperature: – 0°C to +40°C
Relative humidity: Up to 93% (non-condensation)
Exceeding the recommended operating, storage and transportation conditions may result in reduction of the performance of the sensor and/or accessories.
Environment (LWA and Flex Electrode)
Enclosure protection degree: IP21 (when the sensor is connected to a compatible LWA or Flex Electrode)
Operating conditions
Temperature: +5°C to +40°C
Pressure: 700 - 1060 hPa
Relative humidity: 15% – 93% (non-condensation)
Storage conditions (including between uses)
Temperature: 5°C to +27°C
Relative humidity: Up to 93% (non-condensation)
Transportation conditions
Temperature: – 0°C to +40°C
Relative humidity: Up to 93% (non-condensation)
Exceeding the recommended operating, storage, and transportation conditions may result in reduction of the performance of the sensor and/or accessories.
System requirements
The sensor requires a standard computer with the following minimum specifications to read out the recorded data:
- Microsoft® Windows 7 or Mac OS X 10.7 by Apple Inc.
- 1.5 GHz processor
- 512 MB RAM
- USB 2.0 port for connection of the sensor charge adapter USB cable
- 1 GB of free hard-drive space
Validated accessories
The sensor is used in combination with other medical accessories specified by Braemar:
- ePatch™ 2.0 LWA
- ePatch™ 2.0 Flex Electrode
- BTP-1000P Patch
- ePatch™ 2.0-compatible ECG electrodes
- Sensor Charge Adapter
- The provided USB power adapter (USB 5.0 VDC, 250 mA)
Compliance with standards
The sensor conforms to the requirements of the quality standard DS/EN ISO 13485 and the council directive 93/42/EEC (amended) concerning medical devices.
The sensor is manufactured by Braemar and the sensor meets the following standards and regulations:
- IEC 60601-1 ed 3.1 Consol. With am1 (2012) Medical electrical equipment - Part 1: General requirements for basic safety and essential performance
- EN 60601-1-2:2007 Collateral standard: Electromagnetic compatibility - Requirements and tests
- EN 62366:2008 Application of usability engineering to medical devices
- EN 60601-1-11:2010 Medical electrical equipment - Part 1-11: General requirements for basic safety and essential performance - Collateral Standard: Requirements for medical electrical equipment and medical electrical systems used in the home healthcare environment
- IEC 60601-2-47:2012 Medical electrical equipment - Part 2-47: Particular requirements for the basic safety and essential performance of ambulatory electrocardiographic systems
- DS/EN ISO 14971:2007 Medical devices - Application of risk management to medical devices
CardioNet, LifeWatch, and BioTel Heart are trademarks of BioTelemetry, Inc.
TERMS AND CONDITIONS OF THE BIOTELEMETRY SERVICE AGREEMENT.
PLEASE READ THIS DOCUMENT CAREFULLY BEFORE ACTIVATING THE MONITOR.
PRIVACY AND CONFIDENTIALITY
Activating monitoring service serves as your electronic signature indicating you acknowledge that you have received a copy of BioTelemetry’s Notice of Confidentiality and Privacy Practices, which is incorporated in this agreement below. This acknowledgment is required by the Health Insurance Portability and Accountability Act (HIPAA) to ensure that you have been made aware of your privacy rights. You give BioTelemetry your consent and permission to communicate with other members of your household, if necessary, with regard to your BioTelemetry service. You also authorize BioTelemetry to provide your monitoring data to your physician and his / her staff and to Emergency Medical Services by phone, e-mail, fax or through secure Internet access. You consent to receiving calls from BioTelemetry and its affiliates or authorized agents on your landline or cellular telephone related to the service or payment related to the service. For example, BioTelemetry or its affiliate or authorized agent may contact you in order to obtain the loaned BioTelemetry Monitoring System (“System”) or seek payment for the value of the System. You understand that such communications may include the use of prerecorded voice messages and/or automatic telephone dialing systems.
ASSIGNMENT OF BENEFITS
I request that payment of authorized health insurance benefits, including Medicare benefits, if I am a Medicare beneficiary, to be made on my behalf to CardioNet, LLC. ( a subsidiary of BioTelemetry, Inc.) for any medical services provided to me by CardioNet. I authorize any holder of medical and/or insurance information about me to release to CardioNet, my health insurance carrier, or the Centers for Medicare and Medicaid Services (CMS) any information needed to determine these benefits or the benefits payable for related services provided under this agreement. This assignment includes all dates of services rendered by CardioNet for all insurance plans. A copy of this authorization will be sent to CMS or my health insurance carrier if requested. The original will be kept on file by CardioNet. I understand that I am fully responsible to CardioNet for any co-payments, co-insurance, deductibles, payments made directly to me by my health insurance carrier for CardioNet services, and, when allowed by law, services notcovered or payable under my health insurance plan. I also understand that activating monitoring services serves as my electronic signature, and that I am accepting financial responsibility as explained above for all payment for services received from CardioNet. By signing this document and/or accepting these terms electronically, I acknowledge that I have received a copy of CardioNet’s Notice of Privacy Practices. This acknowledgment is required by the Health Insurance Portability and Accountability Act (HIPAA) to ensure that I have been made aware of my privacy rights.
SERVICE AGREEMENT
Financial Terms I understand that I am fully responsible and agree to pay for any co-payments, co-insurance, deductibles, all payments made directly to me by my insurer for CardioNet services, and when allowed by law, services not-covered (not payable) under my health insurance plan. I acknowledge that I am financially responsible for the loaned System (sensor, monitor, and accessories), which I am obligated to return to CardioNet upon completion of the service. If I do not immediately return the System, I hereby authorize CardioNet to invoice me for, and agree to pay CardioNet, the value of the Monitoring System and any associated collection costs should collection or legal costs be incurred by CardioNet.
OPERATIONAL NOTICES
I hereby acknowledge that, given the variance in cellular phone coverage and signal strength, the System may not always provide continuous transmission of my ECG rhythm to the Monitoring Center. In the event that there is no cellular phone coverage or adequate signal strength to transmit recorded events, I will move to an area to optimize transmission capability or connect the monitor and base to a direct telephone line as requested. I hereby acknowledge that the System is intended to aid in diagnosis only, and is not designed for prevention or treatment of any event or condition. I agree to immediately discontinue use of the System upon any sign of discomfort or other problems directly related to the System, and to promptly report such discomfort or other problems to BioTelemetry. I give BioTelemetry and its subsidiaries my consent and permission to communicate with other members of my household, if necessary, with regard to my BioTel Heart service. I also authorize BioTelemetry and its subsidiaries to provide my monitoring data to my physician and his /her staff and to Emergency Medical Services by phone, e-mail, fax or through secure Internet access.
NOTICE OF CONFIDENTIALITY AND PRIVACY PRACTICES
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
PROTECTING YOUR HEALTH INFORMATION
BioTelemetry, Inc., together with its family of companies including CardioNet, LLC, LifeWatch Services Inc., Geneva Healthcare, LLC, BioTel INR, LLC, and Telcare Medical Supply, LLC, understands the importance of keeping your health information private. We are required by law to maintain the privacy of health information that identifies you or can be used to identify you. We are also required to provide you with this notice of our privacy practices, our legal duties and your rights concerning your health information. We are required to abide by the terms of this notice currently in effect. We may modify or change our privacy practices described in this notice from time to time, particularly as new laws and regulations become effective. Any changes will be effective for all the health information that we maintain, even information in existence before the change. If we materially modify our privacy practices, you may obtain a revised copy of this notice by contacting us using the information listed at the end of this notice, or by accessing our website at www.gobio.com/patients.
USES AND DISCLOSURES OF YOUR HEALTH INFORMATION
USES AND DISCLOSURES THAT MAY BE MADE WITHOUT YOUR AUTHORIZATION OR OPPORTUNITY TO OBJECT
We may use and disclose your health information, without your authorization, in the following ways:
Treatment: We may use and disclose your health information to provide, coordinate or manage your treatment. For example, we may disclose your health information to a provider who requests this information to treat you.
Payment: We may use and disclose your health information to bill and get payment for health services we provide to you. For example, we may disclose your health information to your health insurance plan to obtain payment for services provided to you.
Health Care Operations: We may use and disclose your health information in order to support our business activities. For example, we may use your health information to conduct quality improvement activities, to engage in care coordination and case management, to conduct business management and general administrative activities, and other similar activities.
Health & Wellness Information: We may use your health information to contact you with information about health-related services or appointment reminders. If you do not wish to receive this type of information, you may request to opt-out of receiving this information by sending an email to [email protected] or calling the phone number provided at the end of this notice.
Research: Under certain circumstances, we may disclose your health information to researchers when their research has been approved by an institutional review board or privacy board that has reviewed the research proposal and protocols to ensure the privacy of your health information.
Death; Organ Donation: We may disclose your health information to a coroner, medical examiner, funeral director or organ procurement organization for certain purposes as necessary for each to carry out their duties. For example, if you are an organ donor, we may disclose your health information to an organ procurement organization as necessary to facilitate organ donation or transplantation. We may disclose your health information to a coroner or medical examiner to identify a deceased person or determine the cause of death.
Public Health and Safety: We may disclose your health information in connection with certain public health reporting activities. For example, we may disclose your health information to a public health authority authorized to collect or receive such information such as state health departments and federal health agencies. We may use and disclose your health information to the extent necessary to avert a serious and imminent threat to your health or safety or the health or safety of others. We may disclose your health information to appropriate authorities if we reasonably believe that you are a possible victim of abuse, neglect, domestic violence or other crimes. We may also disclose your health information to the Food and Drug Administration (FDA) or a person subject to the jurisdiction of the FDA for the purpose of activities related to the quality, safety or effectiveness of an FDA-regulated product or activity.
Required by Law: We will use or disclose your health information when we are required to do so by law.
Process and Proceedings: We may disclose your health information in response to a court or administrative order, subpoena, discovery request or other lawful process.
Law Enforcement: We may disclose your health information, so long as applicable legal requirements are met, to a law enforcement official, such as for providing information to the police about the victim of a crime.
Inmates: We may disclose your health information if you are an inmate of a correctional institution and we created or received your health information in the course of providing care to you.
Military and National Security: We may disclose your health information to military authorities if you are a member of the Armed Forces. We may disclose your health information to authorized federal officials for lawful intelligence, counterintelligence, protection of the President and authorized persons or foreign heads of state and other national security activities.
Workers’ Compensation: We may disclose your health information as authorized by and to the extent necessary to comply with laws relating to workers’ compensation or other similar programs, established by law, that provide benefits for work-related injuries or illness without regard to fault.
Health Oversight: We may disclose your health information in connection with certain health oversight activities of licensing and other agencies, such as audit, investigation, inspection, licensure, or disciplinary actions, and civil, criminal, or administrative proceedings.
Required by the Secretary of Health and Human Services: We may be required to disclose your health information to the Secretary of the United States Department of Health and Human Services to investigate or determine our compliance with certain legal requirements.
National Instant Criminal Background Check System: We may use or disclose your health information for purposes of reporting to the National Instant Criminal Background Check System the identity of an individual who is prohibited from possessing a firearm under 18 U.S.C. 922(g)(4),
Business Associates: We may disclose your health information to persons who perform functions, activities or services to us or on our behalf that require the use or disclosure of your health information. To protect your health information, we require the business associate to appropriately safeguard your information.
To You: We will disclose your health information to you, as described in the Individual Rights section of this notice.
USES AND DISCLOSURES THAT MAY BE MADE EITHER WITH YOUR AGREEMENT OR THE OPPORTUNITY TO OBJECT
Unless you object, we may disclose to a member of your family, a relative, a close friend or any other person you identify, orally or in writing, your health information that directly relates to that person’s involvement in your health care. If you are unable to agree or object to such disclosure, we may disclose such information as necessary if we determine that it is in your best interest based on our professional judgment. We may use or disclose your health information to notify or assist in notifying a family member, personal representative or any other person that is responsible for your care of your location or general condition.
USES AND DISCLOSURES BASED ON YOUR WRITTEN AUTHORIZATION
Marketing: We must obtain your written authorization to use and disclose your health information for most marketing purposes.
Sale of Health Information: We must obtain your written authorization for any disclosure of your health information which constitutes a sale of health information.
Other Uses: Other uses and disclosures of your health information will be made only with your written authorization, except as described in this notice or as otherwise required or allowed by applicable law.
In the event that we ask for your authorization to use or disclose your health information, we will provide you with an appropriate authorization form. Once you’ve given us a written authorization, you can revoke that authorization at any time, except to the extent that we have taken action in reliance on your authorization.
INDIVIDUAL RIGHTS
Access: You have the right to see or get an electronic or paper copy of your health information by submitting a request to us in writing using the information listed at the end of this notice. There are certain exceptions to your right to obtain a copy of your health information. For example, we may deny your request if we believe the disclosure will endanger your life or that of another person. Depending on the circumstances of the denial, you may have a right to have this decision reviewed. We will charge you a fee to cover the costs incurred by us in complying with your request.
Disclosure Accounting: You have the right to an accounting of disclosures of your health information made by us by submitting a request to us in writing using the information listed at the end of this notice. This right only applies to instances when we or our business associates disclosed your health information for purposes other than treatment, payment, health care operations, upon your written authorization, and certain other activities. The right to receive this information is subject to certain exceptions, restrictions and limitations. You must specify a time period, which may not be longer than 6 years. You may request a shorter timeframe. You have the right to one free request within any 12-month period, but we may charge you for any additional requests in the same 12-month period. We will notify you about any such charges, and you are free to withdraw or modify your request in writing before any charges are incurred.
Restriction Requests: You have the right to request restrictions on the use and disclosure of your health information by submitting a request to us in writing using the information listed at the end of this notice. Your request must state the specific restriction requested and to whom you want the restriction to apply. We are not required to agree to these additional restrictions, except we must agree not to disclose your health information to your health plan if the disclosure (1) is for payment or health care operations and is not otherwise required by law, and (2) relates to a health care item or service which you paid for in full out of pocket. If we agree to a restriction, we will abide by our agreement (except in an emergency).
Confidential Communication: You have the right to receive certain communications confidentially. That means you can request that we communicate with you by alternative means or to an alternative location by submitting a request to us in writing using the information listed at the end of this notice. We will accommodate your request if it is reasonable and specifies the alternative means or location. We may also condition this accommodation by asking you for information as to how payment will be handled.
Amendment: You have the right to amend your health information in our records for as long as we maintain the information. You must make a request in writing, using the information listed at the end of this notice, to obtain an amendment. Your written request must explain why the information should be amended. If we agree to amend your health information, we will make reasonable efforts to inform others of the amendment and to include the changes in any future disclosures of that information. We may deny your request if, for example, we determine that your health information is accurate and complete. If we deny your request, we will send you a written explanation and allow you to submit a written statement of disagreement to be appended to the information you want amended.
Paper Notice: If you receive this notice electronically you are entitled to receive this notice in written form. Please contact us using the information listed at the end of this notice to obtain this notice in written form.
Breach: You have the right to be notified if you are affected by a breach of unsecured health information.
QUESTIONS AND COMPLAINTS
If you want more information about our privacy practices or have questions or concerns, please contact us using the information listed at the end of this notice.
If you are concerned that we may have violated your privacy rights, or you disagree with a decision we made about your rights to your health information, you may submit a complaint to us using the information listed at the end of this notice. You may also submit a complaint to the U.S. Department of Health and Human Services.
We support your right to protect the privacy of your health information. We will not retaliate against you in any way if you choose to file a complaint with us or with the U.S. Department of Health and Human Services.
CONTACT INFORMATION
BioTelemetry, Inc.
Privacy Officer
1000 Cedar Hollow Road, Suite 102
Malvern, PA 19355
Telephone: 610.729.7000
Email: [email protected]
Update Effective date: September 3, 2020
I CERTIFY THAT I UNDERSTAND AND AGREE TO THE FOREGOING TERMS AND TO THE FOLLOWING STANDARD TERMS AND CONDITIONS.
- Use of Cardiac Monitoring System (“System”) and access to and use of Monitoring Service (“Service”). Subject to Patient’s compliance with the terms and conditions indicated within this Patient Education Guide (the “Agreement”), BioTelemetry hereby grants Patient a personal, nonexclusive, nontransferable license to use the System and to access and use the features and functions of the Service solely for purposes of monitoring Patient’s heart rate as prescribed by Patient’s physician. Patient expressly acknowledges and agrees that the Service, which is available only by physician prescription, is used solely to assist physicians in diagnosis and treatment, and is not intended for use as an emergency response system for patients who may experience serious or life-threatening medical problems. Patient is aware that cell phone coverage limitations and delays in land-line telephone communications could significantly delay transmission and analysis of patient monitoring data. Patient agrees to contact BioTelemetry immediately if problems are experienced using the system or if signs of physical discomfort occur, and to discontinue use of the system if the physician or BioTelemetry believe service discontinuation is advisable. Patient shall not, in whole or in part, sublicense, provide access to, tamper with, modify, distribute, use in a service bureau or time-sharing capacity, export in violation of applicable laws and regulations, rent, loan, transfer, disassemble, or reverse engineer or create a derivative work of the System or Service. Patient shall not, in whole or in part, transfer or assign this Agreement or any right granted hereunder, except upon the prior written consent of BioTelemetry. Any prohibited transfer or assignment shall be null and void. Subject to the licenses granted herein, as between BioTelemetry and Patient, BioTelemetry holds all right, title and interest in and to the System and the Service including, without limitation, any patents, trademarks, trade secrets, copyrights or other intellectual property rights therein. BioTelemetry reserves all rights not expressly granted to Patient under this Agreement.
- Term and Termination. This Agreement shall commence on the date that BioTelemetry accepts Patient’s enrollment hereunder, and shall continue until terminated by either party as set forth herein. Either party may terminate this Agreement, for any or no reason, upon thirty (30) days’ written notice to the other party, except that this Agreement shall immediately terminate if Patient breaches Paragraph 1 above. Upon any termination of this Agreement, Patient shall immediately discontinue all use of the Service, and shall promptly return the System to BioTelemetry. The limitations in Paragraph 1, and Paragraphs 3-6 shall survive any termination of this Agreement.
- NO WARRANTY. THE SYSTEM AND THE SERVICE ARE PROVIDED BY BIOTELEMETRY HEREUNDER SOLELY ON AN “AS-IS” AND “AS AVAILABLE” BASIS WITHOUT WARRANTY OF ANY KIND. TO THE MAXIMUM EXTENT PERMITTED UNDER APPLICABLE LAW, BIOTELEMETRY HEREBY DISCLAIMS ANY AND ALL WARRANTIES, EXPRESS, IMPLIED OR STATUTORY, INCLUDING, BUT NOT LIMITED TO, ANY WARRANTY OF MERCHANTABILITY, FITNESS FOR A PARTICULAR PURPOSE, TITLE, NON-INFRINGEMENT AND/OR QUIET ENJOYMENT, AS WELL AS ANY IMPLIED WARRANTIES OTHERWISE ARISING OUT OF COURSE OF DEALING, COURSE OF PERFORMANCE OR TRADE USAGE. PATIENT FURTHER ACKNOWLEDGES AND AGREES THAT BIOTELEMETRY SHALL NEITHER BE RESPONSIBLE NOR LIABLE FOR PATIENT’S INABILITY TO ACCESS OR USE THE SERVICE AS A RESULT OF ANY DEFICIENCY IN THE INTERNET, THE TELEPHONE SERVICE, OR OTHER CONNECTION BETWEEN BIOTELEMETRY AND PATIENT. PATIENT EXPRESSLY ACKNOWLEDGES AND AGREES THAT NEITHER THE SYSTEM, NOR THE SERVICE (AS WELL AS ANY SUPPORT GIVEN BY ANY BIOTELEMETRY SUPPORT STAFF), NOR ANY MATERIAL AVAILABLE THROUGH PATIENT’S USE OF THE SYSTEM OR SERVICE IS INTENDED TO PROVIDE PATIENT WITH MEDICAL ADVICE, A DIAGNOSIS OR TREATMENT. PATIENT MUST ALWAYS SEEK THE ADVICE OF PATIENT’S PHYSICIAN OR OF ANOTHER QUALIFIED MEDICAL PRACTITIONER WITH ANY QUESTIONS PATIENT MAY HAVE REGARDING A SPECIFIC MEDICAL CONDITION OR PERCEIVED CONDITION.
- LIMITATION OF LIABILITY. TO THE MAXIMUM EXTENT PERMITTED UNDER APPLICABLE LAW: (I) IN NO EVENT SHALL BIOTELEMETRY OR ITS SUBSIDIARIES, AFFILIATES, OFFICERS, DIRECTORS, EMPLOYEES AND AGENTS, ITS LICENSORS OR SUPPLIERS BE LIABLE TO PATIENT FOR ANY INDIRECT, INCIDENTAL, SPECIAL, CONSEQUENTIAL OR PUNITIVE DAMAGES ARISING OUT OF OR RELATED TO THIS AGREEMENT INCLUDING, WITHOUT LIMITATION, LOST PROFITS, COSTS OF DELAY, ANY FAILURE OF DELIVERY, BUSINESS INTERRUPTION, COSTS OF LOST OR DAMAGED DATA, UNAUTHORIZED DISCLOSURE TO OR ACCESS OF PATIENT DATA, OR LIABILITIES TO THIRD PARTIES ARISING FROM ANY PERSONAL INJURY OR PROPERTY DAMAGE CLAIM OR ANY OTHER TYPE OF CLAIM, EVEN IF BIOTELEMETRY HAS BEEN ADVISED OF THE POSSIBILITY OF SUCH DAMAGES; AND, (II) IN NO EVENT SHALL BIOTELEMETRY’S AGGREGATE LIABILITY UNDER THIS AGREEMENT EXCEED THE AMOUNT PAID BY PATIENT TO BIOTELEMETRY UNDER THIS AGREEMENT. THE PARTIES AGREE THAT THE ALLOCATION OF LIABILITY SET FORTH IN THIS SECTION 5 FORMS AN ESSENTIAL BASIS OF BIOTELEMETRY’S WILLINGNESS TO GRANT PATIENT THE USE OF THE SYSTEM AND ACCESS TO AND USE OF THE SERVICE AND IS INDEPENDENT OF EACH AND EVERY LIMITED REMEDY THAT PATIENT MAY HAVE.
- Indemnity. Patient agrees to indemnify and hold harmless BioTelemetry, Inc., it’s subsidiaries, and its officers, directors, employees, agents and suppliers from and against all claims of third parties arising out of or related to Patient’s use or misuse of the System and/or the Service, or attributable to Patient’s breach of this Agreement. BioTelemetry shall control the defense and any settlement of such claim, and Patient shall cooperate with BioTelemetry in defending against such claims.
- General Provisions. This Agreement may be modified or amended only by a written instrument signed by Patient and BioTelemetry. Any terms and conditions issued by Patient shall not be binding on BioTelemetry, Inc., or it’s subsidiaries, officers, directors, employees, agents or suppliers, and shall not modify these Terms and Conditions. No term or provision contained herein shall be deemed waived and no breach excused unless such waiver or consent shall be in writing and signed by the party against whom enforcement thereof is sought. Neither party hereto shall be liable to the other for any failure to perform its obligations under this Agreement due to causes beyond the reasonable control of that party, including, but not limited to, strikes, boycotts, labor disputes, embargoes, unavailability of or failures due to telecommunication networks (including, without limitation, the Internet), acts of God, unavailability of or insufficient utilities, acts of public enemy, acts of governmental authority, floods, riots, or rebellion. This Agreement shall be governed by and construed solely in accordance with the laws of the State of Pennsylvania, without reference to its choice of law rules. Any and all proceedings arising under or in any way relating to this Agreement shall be maintained in the state or federal courts located in Chester County, Pennsylvania, which courts shall have exclusive jurisdiction for such purpose, and Patient hereby consents to the personal jurisdiction of such courts. Patient acknowledges that in the event of an actual or threatened violation of the terms and conditions of this Agreement, BioTelemetry may not have an adequate monetary remedy and shall be entitled to seek injunctive relief without any requirement to post bond, in addition to any other available remedies. If any term or provision of this Agreement is illegal or unenforceable, it shall be deemed adjusted to the minimum extent to cure such invalidity or unenforceability and all other terms and provisions of this Agreement shall remain in full force and effect.
IMPORTANT REMINDER:
This device provides a diagnostic test. It is not an emergency response service.
If at any time you experience a symptom that you feel is a medical emergency, you should immediately dial 911 for medical assistance.
1000 Cedar Hollow Road, Malvern, PA 19355
Toll free: 1-877-593-6421 • [email protected] • www.myheartmonitor.com
Copyright © 2021. All rights reserved. Doc. 220-0690-01 Rev. C